Cities / Healthy Cities
A blueprint for healthy and resilient cities
By Kate Ardern, Derek Clements-Croome, Emily Loquidis and Sotiris Vardoulakis | 13 Feb 2018 | 0
This paper will discuss how the implications of the authors’ various work can be translated into developing specific solutions for cities, focusing on challenges around mobilisation, inclusive design, and benchmarks for progress.
Authors of scientific paper:

Abstract
In 2016, an estimated 54.5 per cent of the world’s population lived in urban settings with this figure projected to grow to 60 per cent by 2030.1 As cities grapple with the environmental and health issues associated with population growth and urbanisation, there is an increasing trend towards people-centric design, focused on health and wellbeing. A healthy city should be one designed for all its citizens – inclusive, supportive, sensitive and responsive.
The paradigm shift to support a society of wellbeing requires a blueprint for a healthy city that takes into consideration urban resilience through government support, public health, building design, and the intersection of technology as a tool for data feedback and measurement. Greater Manchester – energised by their pioneering devolution programme, together with the work of their civil contingencies and resilience unit, and the high-profile support of collaborators such as the United Nations International Strategy for Disaster Reduction (UNISDR) and 100 Resilient Cities – is one city (or metropolitan area) working hard to integrate wellbeing, health and social care to create sustainable, resilient neighbourhoods and a social movement for change driven by citizen empowerment.
Pressure from climate change, weather extremes, and air pollution on urban populations presents both a public health challenge and a design opportunity. Healthy Polis, an international consortium for urban environmental health and sustainability, details new work around health challenges related to air pollution and climate change in cities by focusing on the wider co-benefits and consequences of urban planning policies and interventions. These co-benefits (or resilience dividends) are also a primary focus for actions being promoted through the 100 Resilient Cities programme.
In thinking about healthy cities, we need to address all scales – from a whole-of-city strategic vision, through to neighbourhoods and individual buildings. While buildings traditionally provide comfort and protection from external threats, we’re increasingly discovering health risks associated with our internal environments. The WELL Building Standard is the first building certification system that focuses exclusively on human health and wellness. AECOM outlines the implementation of WELL on one of the first projects in the UK, and explains how sustainability and wellbeing goals were integrated and executed alongside considerations of broader organisational wellbeing policy. The criteria in new standards such as WELL have shifted the definition of good practice, which also means that occupants will adopt a new baseline expectation. Research from the University of Reading, in collaboration with the British Council for Offices, investigates the use of wearable technology and how this data can act as a fundamental feedback loop to inform the planning and design of intelligent buildings and healthy cities of tomorrow.
This paper will discuss how the implications of this work can be translated into the development of specific solutions for cities, focusing on challenges around mobilisation, inclusive design, and benchmarks for progress.
Keywords
Cities are complex organisms that require holistic, system-based approaches to address challenges and harness opportunities for improving health and wellbeing. The complexity of cities is related to the multitude of inter-connected economic, social, environmental and infrastructure aspects that need to be taken into account in local decision-making.
The siting and design of new buildings, facilities and estates, for example, could reduce the need for motorised travel and minimise exposure to air pollution, particularly among vulnerable groups. This can be achieved by not siting schools, nurseries and care homes in areas where exposures are likely to be high.2 Furthermore, providing infrastructure for cycling and walking can reduce the number of short car journeys, improving local air quality and physical activity levels.
A recent modelling study has looked at how sensitive receptors, such as hospitals and care homes, in Birmingham (West Midlands, UK) respond when exposed to heat during heatwaves. The models compared temperatures at these locations with average temperatures across the region. The study found that hospitals and care homes were exposed to higher ambient temperatures than average, and that housing types more likely to overheat were located in the warmest parts of the city.3 Further analysis of relative deprivation across the region indicated that more deprived populations live in the warmest parts of the city.
In the residential sector, measures aimed at reducing carbon emissions have the potential to provide additional health benefits, including reductions in heat and cold health effects, and indoor exposure to air pollution derived from outdoor sources. However, increasing airtightness of dwellings in pursuit of energy efficiency could also have negative effects by increasing concentrations of indoor pollutants. These effects can largely be ameliorated by mechanical ventilation with heat recovery (MVHR) and air filtration, where such a solution is feasible and when the system is properly installed, operated and maintained.4 A better understanding of how current and emerging building infrastructure design, construction and materials may affect health in the context of climate change is needed.
Citizen science approaches based on smart sensors, mobile phones and other portable devices can generate “big data”, including environmental, health and socioeconomic data from cities.5 This is an opportunity and a challenge to ensure the quality of the data, and analyse it in a meaningful way that leads to actionable outcomes.
These challenges and opportunities highlight the need for integrated system-based assessment methods that account for the complex interactions between climatic, environmental, socio-economic, and behavioural factors, and the urban fabric. This is the approach adopted by Healthy-Polis (www.healthy-polis.org), an international consortium for urban environmental health and sustainability, which aims to: promote innovation and standardisation in research methods (including exposure modelling, environmental epidemiology, risk analysis and communication); facilitate international, multidisciplinary research collaborations; provide training and promote capacity building, especially in rapidly urbanising countries; and evaluate and promote environmental interventions to improve public health in cities.6
Health and resilience implementation in Greater Manchester
Greater Manchester’s devolution offers a huge opportunity for a place-based approach to public health leadership by addressing interlinked health determinants to embed “health in every policy” and improve health outcomes at pace and scale. Cities are increasingly recognising the benefits of integrated service delivery; however, these services need time and expertise to shift thinking from traditional service provision and ways of working.
In order to shepherd this reform, a single Greater Manchester Strategy was developed that focuses on broad, public health-sector principles, driven by an evidence-led understanding of risk and impact, integrated asset implementation, and behaviour-based change through a place-based approach.
Building on this framework, a health and social care vision to deliver the greatest and fastest possible improvement to the health and wellbeing of the 2.8m people in Greater Manchester was defined, as follows:
- create a transformed health and social care system that helps more people stay well and takes care of the ill;
- align the health and social care system comprehensively to education, skills, work and housing;
- create a financially balanced and sustainable system; and
- ensure the system remains clinically safe throughout.
The vision is to be delivered at four spatial levels – Greater Manchester; cluster; locality; and neighbourhood. Each level works to deliver the objectives through a range of improvement programmes while identifying that some reform cannot be delivered within existing resources or through existing efficiency plans. Goals are defined at developmental phases for the community – from starting healthy at birth to living and ageing well. 
Each sector also identifies key risks to health and wellbeing and how to offset these risks through community services; for example, Wigan Borough identified risks for the community, including debt, poor housing and social isolation. In response to these risks, the borough has pledged to provide training and job opportunities, quality housing, connection to the community, and quality health services that are accessible and sustainable. Services delivery alone cannot improve health and wellness; a sense of civic responsibility around wellness is also being fostered by “The Deal” – an informal agreement between the council and everyone who lives or works in the borough to work together to build a better place to live. Residents can sign up to recycle more, for example, or be healthy and active.7
Greater Manchester’s efforts to repair systemic challenges are supported by examining potential stresses to community in line with the 100 Resilient City’s Initiative. The initiative is dedicated to helping cities around the world become more resilient, including not just the shocks – earthquakes, fires, floods – but also the stresses that weaken the fabric of a city and its people on a day-to-day cyclical basis. Greater Manchester faces environmental challenges such as flooding, which has the potential to disrupt government services and damage crucial infrastructure. Deprived communities living in flood-risk areas are at the greatest risk and already face a growing economic burden in the form of higher insurance premiums. Greater co-ordination among local authorities has increased the city’s ability to respond effectively to emergencies, while partnerships with public and private stakeholders have helped the city better identify the potential impacts of climate change.8
Systemic change and planning for resiliency requires appointing staff with energy and motivation to support transformation. It’s also crucial to empower citizens as equal partners in improving health and community resilience. We must stop viewing public health through the lens of a small clinical specialty and see it as a fully integrated local government function, influencing and supporting both the civic and the public’s leadership at the core of public service reform.
Wellbeing in the built environment
While buildings traditionally provide comfort and protection from external threats, we’re discovering health risks associated with our internal environments. With people now spending 90 per cent of time indoors, it’s evident that we must design, construct and operate buildings that are both sustainable and healthy.9
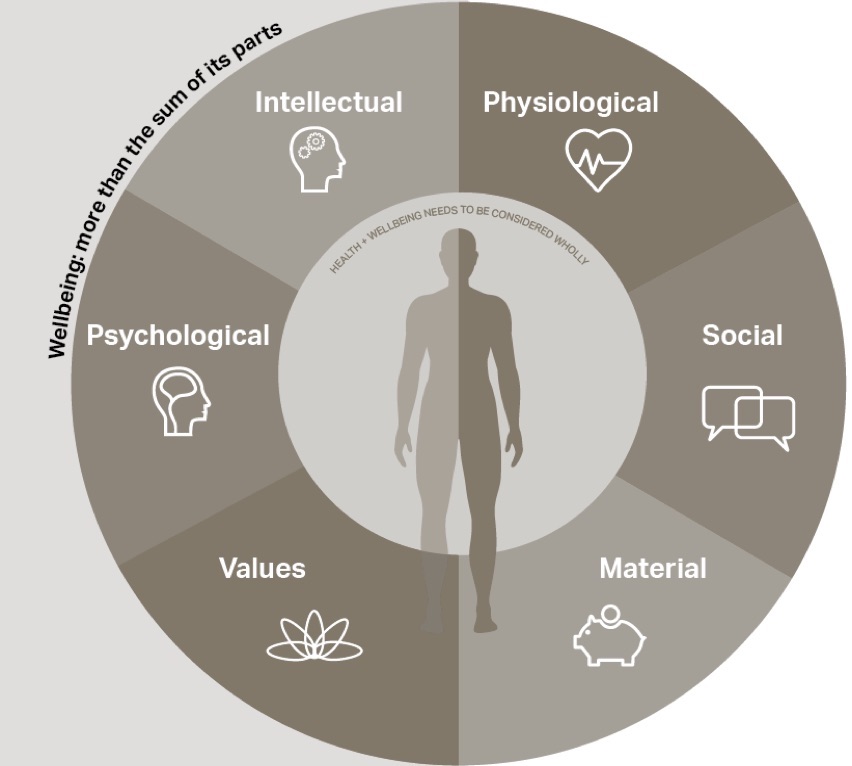
While it’s important that organisations become more environmentally friendly, the major cost inside buildings is people – the bulk of typical business operating costs are related to staff costs and salaries.9 It follows that the health and productivity of staff will be the primary focus for most organisations. This focus drives consideration of improvements to the physical space but also goes deeper to explore how wellbeing permeates organisational culture through policies such as talent strategies, total reward plans, and employer relations. Wellbeing is a complex concept that requires a multidisciplinary approach and intervention throughout the organisation.
 Going beyond “green” means promoting health and wellbeing through high-performance building design that identifies ways to jointly meet sustainability goals and support occupant health and wellbeing. Lighting design, for example, can be a challenge to balance energy efficiency goals alongside circadian lighting health and occupant comfort.
Going beyond “green” means promoting health and wellbeing through high-performance building design that identifies ways to jointly meet sustainability goals and support occupant health and wellbeing. Lighting design, for example, can be a challenge to balance energy efficiency goals alongside circadian lighting health and occupant comfort.
Circadian rhythms are kept in sync by various cues, including light, which the body responds to in a way facilitated by intrinsically photosensitive retinal ganglion cells (ipRGCs), the eyes’ non image-forming photoreceptors.10 Through ipRGCs, lights of high frequency and intensity promote alertness, while the lack of these stimuli signals the body to reduce energy expenditure and prepare for rest. The biological effects of light on humans can be measured in Equivalent Melanopic Lux (EML), a proposed alternate metric that’s weighted to the ipRGCs instead of to the cones, which is the case with traditional lux.10
One such project, an office refurbishment project in central London, addressed these goals by installing an energy-efficient LED lighting system, which also had high EML levels in the space. Upon occupancy, surveys were conducted to measure occupant satisfaction, as well as rigorous performance testing of the EML levels in the space. Interestingly, the installation was able to pass benchmarks established by the WELL Building Standard in the upper ranges of lux levels; however, occupants complained of high glare when the lighting system was addressed at the maximum and was ultimately commissioned to operate a lower range. Flexibility in this case came in the form of task lighting; individuals used these, in addition to the overhead lights, to provide a broad spectrum of light at the working plane that could be adjusted to two levels of brightness. This example underpins the importance of flexibility in the lighting system to respond to the comfort of current and future occupants.
The criteria in new building standards have shifted the definition of best practice, which also means that occupants will adopt a new baseline expectation. The increasing availability of affordable monitoring equipment and wearable technology allows occupants to be aware of their internal environments and empowers them to challenge organisations on the quality of internal spaces, in addition to taking personal steps to tracking movement, diet, and limiting screen time.
With health and wellbeing envisaged as the next trillion-dollar industry, the trend towards people-focused design will only grow.11 The challenge will be to ensure that the larger wellbeing principles are embraced by the market to become standard best practice and inclusive for all – not merely for a lucky few who can live and work in healthy and sustainable buildings and communities.
The digital city
The digital city is a specific term referring to the information and computing technologies embedded into the design and operation of cities to enable seamless communications for organisations, individuals and communities. Social media, the internet, cloud computing, sensors, and mobile phones are creating a digital infrastructure (SMART 2020) to build a sentient city – one that responds to the needs of individuals and communities, and supports the health and wellness of its citizens.
Cities comprise a number of interacting systems, which can present inherent friction to integrate digital solutions and hinder a city’s effort to make itself “smart”. Some systems can be modelled more easily than others to determine potential conflict. Modelling a transport system, for example, is possible but the impact on business and social consequences is more difficult to forecast. Forkenbrock and Weisbrod (2001) note that transport networks can affect an area’s visual quality, level of traffic noise, air pollution, social interactions, and community cohesion – all of which can affect an area’s ability to attract new businesses and residents. Interoperability within the system is vital.
The digital city can take many forms – from smart infrastructure integration to improvements in computing technology. The Digital Cities Survey 2016, for example, is a US-based survey that recognises leading examples of cities using technology to improve services, boost efficiencies, and increase government transparency and citizen engagement. Los Angeles was included in the 2016 list of finalists on the survey for its efforts to integrate sustainability, collaboration, mobility, cybersecurity and open government. The city recently built an extensive open data portal, and helped launch 34,000 new businesses, as well as work toward digital inclusion.12 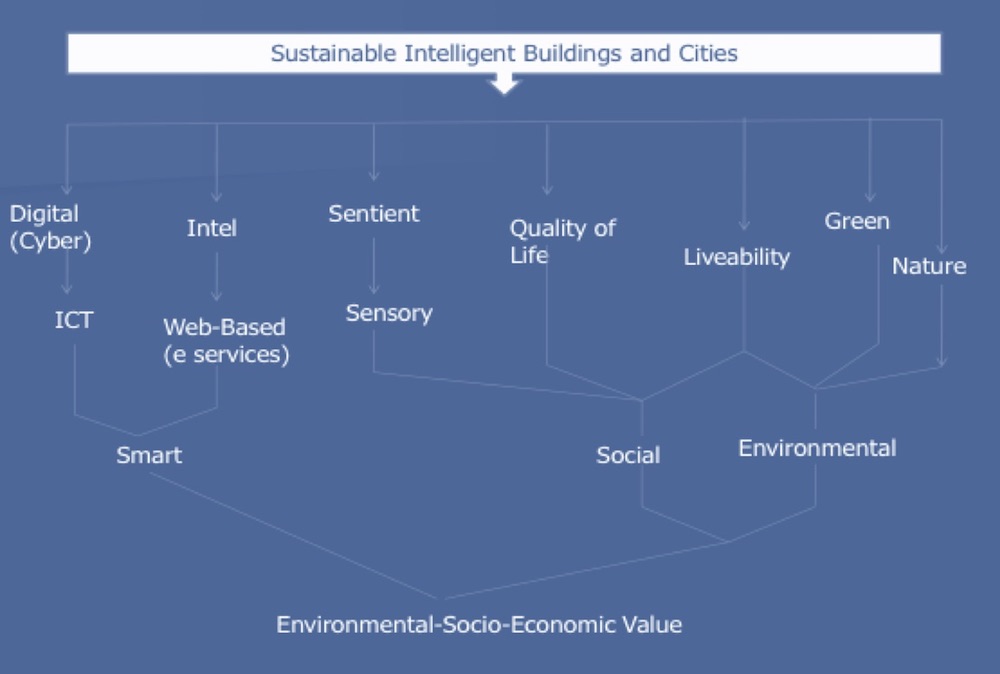
Increasingly, we see sensors being embedded in materials, including clothing, so people become part of a wireless sensor network. Not only can physiological responses be measured but also moods and stress levels. Wearables are creating an increased sense of health and wellbeing, and these have the potential to integrate more directly with the healthcare system. Data from wearables, for instance, could link to online data portals for doctors, leading to early diagnosis of health issues and promoting preventive care. In addition to privacy concerns, personal digitisation faces other challenges, such as making sense of and interpreting data correctly, identifying impactful tools in a market susceptible to gimmicks, and conducting regular updating of devices such as smartphones and computers.13
Embedding technology into the built environment is another way to integrate digitisation to support health and wellbeing in cities. Examples can be found in the infrastructure and public realm elements of the city, as well as in buildings themselves. The Cybertexture Egg, designed by James Law and currently being constructed in Mumbai, is one such building integrating technology, multimedia, intelligent systems and user interactivity to create customisable living and working spaces. The operation of the building takes this principal working theme a step further with interactive features that monitor occupants’ vital health statistics, such as blood pressure and weight. In keeping with the focus on health and wellness, users can customise their views with real-time virtual scenery. The building also combines people-focused design with sustainability features, such as incorporating passive solar design to decrease heat gain, lower energy loads, and promote occupant comfort. An elevated garden also moderates temperatures by using natural vegetation to assist with cooling the building envelope.14
The future drivers for the digital city exist today and will increase in application through cities: digital, sustainable, smart and nano technologies, along with robotics, sensor integration, 3D and 4D printing, and biomimetic architecture.15 The digital city must demonstrate socio-economic value, in which quality is sought for a whole-life cost, to ensure that digitisation is managed with emphasis on people.
Conclusion
Many pressures aside from technological development will influence the built environment. There will be impact from climate change, environmental, demographic, and social change around how the way buildings are designed, built and operated. Cities are comprised of infrastructure and buildings, but they must also rely on the organisational, managerial and policy aspects that make the decisions for that city. Because of the complex number of interacting systems that define a city, improving health and wellbeing of citizens can be a daunting task.
Cities will need to trial innovative solutions, both at the policy level, as the Manchester example highlights, and through design solutions and climate change mitigation. Increasingly, tools such as the WELL Building Standard, will begin to serve as a benchmark for progress. The city, as a whole, has boundaries set by nature. Time, in the sense that the city is for both present and future generations, will continue to be a focus in order to build and operate communities that are sustainable and healthy.
Authors
Professor Kate Ardern is executive director at Public Health Wigan; Derek Clements-Croome is professor emeritus at the University of Reading; Emily Loquidis is principal consultant at AECOM; and Dr Sotiris Vardoulakis is research director at Healthy Polis.
References
- The United Nations. The world’s cities in 2016; 2016.
- NICE (National Institute for Health and Care Excellence). Air pollution: outdoor air quality and health. NICE. Public Health Guideline NG70; 2017. Available at: https://www.nice.org.uk/guidance/ng70
- Macintyre, HL, Heaviside, C, Taylor, J, Picetti, R, Symonds, P, Cai, X, Vardoulakis, S. Assessing urban population vulnerability and environmental risks across an urban area during heatwaves – implications for health protection. Science of the Total Environment, 610–611, 678-690; 2018.
- Vardoulakis, S, Dimitroulopoulou, S, Thornes, JE, Lai, K-M, Taylor, J, Myers, I, Heaviside, C, Mavrogianni, A, Shrubsole, C, Chalabi, Z, Davies, M, Wilkinson, P. Impact of climate change on the domestic indoor environment and associated health risks in the UK. Environment International, 85, 299–313; 2015.
- Fleming, LE, Haines, A, Golding, B, Kessel, A, Cichowska, A, Sabel, CE, Depledge, M, H, Sarran, C, Osborne, NJ, Whitmore, C, Cocksedge, N, and Bloomfield, D. 2014. Data mashups: potential contribution to decision support on climate change and health. Int J Environ Res Public Health, 11(2): 1725–46.
- Vardoulakis, S, Dear, K, and Wilkinson, P. Challenges and opportunities for urban environmental health and sustainability: the Healthy-Polis initiative. Environmental Health, 15(1): 1–4; 2016.
- Wigan Council. ‘What is the deal?’; www.wigan.gov.uk. Accessed 27 September 2017.
- 100 Resilient Cities. ‘Greater Manchester’s resilience challenge’; www.100resilientcities.org. Accessed 27 September 2017.
- World Green Building Council. ‘Health, wellbeing and productivity in offices: the next chapter for green building’; 2014.
- International WELL Building Institute. ‘The Well Building Standard, Feature 54. Circadian Lighting Design’; March 2017.
- McKinsey and Company. ‘Healthy, wealthy and [maybe] wise: the emerging trillion-dollar market for health and wellness; May 2012.
- Digital Cities. ‘Digital cities survey 2016 – winners announced’; http://www.govtech.com/dc/digital-cities/Digital-Cities-Survey-2016-Winners-Announced.html. Accessed 28 September 2017.
- Clements-Croome, Derek. ‘Intelligent, liveable buildings for the 21st century’. University of Reading Intelligent Buildings International; 2017.
- Inhabit. ‘Cybertexture egg for Mumbai’; www.inhabit.com. Accessed 28 September 2017.
- Clements-Croome, Derek. ‘Intelligent buildings: design, management and operation.’ Thomas Telford Publishing, 2004.
Organisations involved