Senior care / Quality improvement
Architecture for Alzheimer’s disease
By Catarina Oom | 29 Aug 2018 | 0
The project, Architecture for Alzheimer’s disease, seeks to understand the influence of the physical and sensory environment on the lives of Alzheimer’s patients and their caregivers.
Author of scientific paper:

Abstract
Objectives: In this paper, we seek to understand the influence of the physical and sensory environment in the daily life of an Alzheimer’s patient, and those who live with and care for these patients. It’s intended to establish therapeutic objectives as guides to define the relationship between people with dementia and their environment, based on their challenging behaviours, by proposing possible architectural solutions.
Methods: The project started with an extensive bibliographic research in order to study the disease, and through meetings with health professionals, along with the experience and contact with patients, carers and families. After identifying the challenging behaviours associated with the disease, the physical characteristics of the environment contributing to the softening of behaviours, and thereby promoting calm and wellbeing, were analysed. The concept of the atmosphere and its connection to memory was then reflected on in order to create a familiar, comfortable, recognisable and stimulating atmosphere, appropriate to the disease progression stage of each patient.
Results: For Alzheimer’s patients, most of whom are elderly, the requirements related to old age are added to others, such as the need to: ensure safety; create flexible and adaptable environments to the change of wills and capacities; maximise autonomy and control; contribute to an easier finding of the way; promote stimulating and meaningful activities; provide contact with nature; foster opportunities for establishing positive social relationships; encourage family involvement; elevate carers and health professionals; and, finally, provide a “feeling of being at home” by stimulating memories, playing with illumination and colour, and facilitating contact with religion and spirituality. Being a disease with different stages of progression, it’s important to have in mind the difference between patients’ cognitive and motor skills, and to provide the right level of stimulation in each case.
Conclusion: The environment and atmosphere experienced by patients, carers and family members have a direct influence on daily living. Contact with patients, and the possibility of getting to know the future user of the space that we’re designing are key to evidence-based architecture centred on real people. This allows the possibility to create a healthy environment, adapted and human for people who will inhabit this space until the end of their lives.
Keywords
Introduction: architecture and health
In the last few decades, growing awareness that space affects mood and behaviour, and hence health, has helped architects design places that relate to the human body in order to maintain health and promote healing instead of increasing stress and disease.1 Awareness that the healthcare environment is a powerful place and can be considered a “stage” in the healing journey2 has resulted in the popularity of two concepts of great importance: evidence-based design and supportive design.
Evidence-based design helps people take design decisions according to the best available current research evidence.3 The theoretical study of the presented subject, together with knowledge of the objective reality of the future user of the space, gives the architect the necessary tools to design a project based on evidence and, consequently, meet the real needs of the population.4
The theory of supportive design refers to the environmental characteristics that support or facilitate the management of stress that accompanies illness and hospitalisation.5 The process begins by eliminating the environmental characteristics known as stressors or that may have negative impacts on the results, such as noise. This type of architectural design also goes a step further by emphasising that the inclusion of certain characteristics and opportunities in the environment has a reassuring effect on patients, reduces stress, and strengthens the healing processes. The proposed guides to create these environments are to increase control, privacy, promote social support, and allow access to nature and positive distractions.
Alzheimer’s disease
Alzheimer’s disease is a neurodegenerative disease of unknown cause that mainly affects the elderly. The main – and usually the first – clinical manifestation of this disease is memory impairment. Although there are treatments available that can improve some of the symptoms, there is no cure or therapy to stop the disease from developing, and it inevitably progresses in all patients.6
The project ‘Architecture for Alzheimer’s disease’ seeks to understand the influence of the physical and sensory environment in the daily life of an Alzheimer’s patient, and those who live and care for these patients on a daily basis.
There are two main reasons to focus on Alzheimer’s disease: the first is the increase in average life expectancy and consequent ageing. Based on a recent study,7 the global average life expectancy in 2015 was 65 years, and within 15 years, this figure will increase by five years. Moreover, the number of people over 85 worldwide in 2050 will exceed 20 million. Growing older is associated with a series of difficulties or behaviours specific to this phase of life. However, older people eventually develop some form of dementia. Alzheimer’s disease –the most common type of dementia (60-70 per cent of cases) with an age-dependent incidence – appears as a topic of great importance in different areas of human knowledge and society in general. As the global population ages, the number of people living with dementia is expected to triple from 50 million to 152 million by 2050.8
The second reason to focus on Alzheimer’s is it offers an opportunity to study the therapeutic capabilities of architecture, and understand the needs of the future user of the space in order to design based on evidence. Spending time at a special care unit (SCUA) conceived for people with Alzheimer’s was an opportunity to meet patients, carers and relatives, and a chance to learn about the challenges this issue poses for architecture.
Symptoms
A literature review was conducted on the relationship between the design of the built environment and the impact on people with dementia.9 The aim of this literature review was to define the typical behaviours of dementia that may be affected by interventions in the environment. The results of this study indicate that while behaviours related to function (daily activities, mobility), wellbeing (depression, mood), behaviour (agitation, aggression, apathy, anxiety), social (interaction), orientation (wayfinding) and medical outcomes (medication reduction, improvement in sleep) are influenced by the architectural design, cognitive aspects (attention, cognitive performance) do not appear to be affected by environmental interventions.
Based on these findings,9 in the challenging behaviours defined by Elisabeth Brawley10 in the medical publication Up to Date,6 and through contact with patients and carers at the SCUA, the characteristic symptoms of Alzheimer’s disease in which architecture can have a beneficial impact were defined as: memory loss; disorientation; wandering; difficulty in carrying out day-to-day tasks; incontinence; intent to leave; sleep disturbances; agitation; anxiety; aggression; and apathy.
Therapeutic objectives
These person-centred goals intend to promote the guidelines for the creation of appropriate and supportive environments. These are guides to define the relationship between people with dementia and their environment based on their challenging behaviours.
Guarantee security
Safety is one of the main concerns of residents and their families when it comes to changing their own home for an assisted living unit.11 There are two types of security: one that really exists and one that’s perceived. It’s not only important that residents are safe but that they also feel safe. The physical environment must provide both types, thereby giving confidence to the residents.12
The security that really exists includes a series of precautions, such as preventing access to toxic substances and dangerous objects, preventing falls, allowing carers to observe residents, and preventing them from leaving.10 Perceived security relates to the choices of materials. Surfaces with too much reflection are a cause of discomfort, insecurity and often panic on the part of residents.
In an Alzheimer’s facility, all the main activities should be developed on the same level with minimum changes to floor elevation, and the spaces must be visible even for those who are outside the activity rooms by way of transparent materials on the corridor wall.13 The amount of light and existence of a clear path through the house with stable furniture are possible strategies to prevent falls. Bathrooms shared by two rooms facilitate control and maintain safety by reducing the areas of greatest danger. Here, adding high-contrast, slip-resistant material to flooring increases safety. Furthermore, amber-coloured LEDs (which do not disturb circadian rhythm) in the bathroom or around the bathroom doorway create a clear path from the bed to the toilet, preventing falls during the night.14
The Dutch half doors, used in the home of the elderly De Drie Hoven of Herman Hertzberger, are a possible solution for rooms, allowing, among other things, carers and professionals to observe what happens inside, and control the security of each resident without invading their privacy or risking their independence.
Alzheimer’s disease patients have reduced contrast perception ability, meaning they need higher visual contrast to maximise function. The floor should have a minimal or low-contrast patterning, and the floor and wall should have appropriate contrast. Of great concern should be the avoidance of creating dead ends at the end of corridors, and minimising the number of doors, which should be the same material as the walls in order not to attract attention and invite use.
It’s important to bear in mind that having a diagnosis does not mean the person is at risk of walking away and should be locked inside. The control of safety should always be balanced with autonomy and choice.
Adaptation to changing needs
It’s important to remember that no two patients with dementia are the same. Every person who enters an assisted home has lived a unique life with experiences that have resulted in different interests, capacities and values. It’s important to recognise the abilities of each person, and this should contribute to a programme that treats each person as an individual with respect and dignity.11 Moreover, Alzheimer’s disease and other types of dementia progress in different ways, going through different phases with specific needs. For this reason, it’s important to take into account not only the differences and capabilities in residents themselves but also the changing needs of each person as the disease progresses. The behaviours exhibited in early-stage dementia patients are very different from late-stage patients, and early-stage patients don’t want to be around the behaviours of those at a more advanced phase.15
The concept of age in place was also studied, whereby the architectural environment is shaped to an individual’s needs without a change of the physical space – allowing a resident to inhabit the same room until the end of their life.11
One possible way to personalise care is to divide rooms into different households. These households could have between six and 12 residents (with two or three households in the building). Each household should have a kitchen, dining room, living room and activity rooms, and each should provide direct contact with outdoor gardens and walking paths.14 These households should be designed according to the degree of development of the disease and associated limitations, functioning as small families where the activities can be carried out in a small group. What differs between these households is the type of rooms, the relationship with the outside, and the stimulus to which the residents are exposed.
All the rooms, regardless of the household, should contain characteristics that allow the disease to evolve. The entrance door to the room, for example, has two leaves that can be adapted according to the development of the disease and the need to move the bed; the entrance to the bathroom should always allow for movement of the bed to the inside; and all the mirrors should be hidden since, during development of the disease, these can become frightening. At the SCUA, it was obvious that the people were afraid of the mirror because they didn’t recognise the reflected person they saw.
In all households, the majority of bathrooms should be shared. But there should be rooms with an individual bathroom for people who retain their physical and cognitive abilities.
In households designated to patients in an early and intermediate phase of the disease, there should be a diversity of activity options – for example, raised plant beds to encourage gardening activities. For more dependent patients, more rooms should be available for sensory stimulation, while consideration should be given to the possibility of moving the resident’s bed to a protected exterior.
Maximise autonomy and control
Residents with dementia are generally better able than their carers know or expect. When day-to-day activities are simplified, distributed in small spaces, or adapted to meet their needs, residents can be more independent for longer.10
Dressing, for example, is a complex activity that requires significant decision-making skills. The wardrobe of the room can be divided into two compartments, the larger one being used to organise the resident’s clothes, with the smaller one containing only the specific clothes for that day. These pieces of clothing are sorted out by an assistant the day before they are to be worn (in the order they should be put on) to support independence and autonomy while avoiding confusion and frustration.
 In addition, the existence of a kitchen counter, an accessible area of laundry, and a private outdoor space allows each resident to perform activities of daily living, such as cooking, washing clothes or watering plants, for as long as possible.
In addition, the existence of a kitchen counter, an accessible area of laundry, and a private outdoor space allows each resident to perform activities of daily living, such as cooking, washing clothes or watering plants, for as long as possible.
Wayfinding
Finding your way is a prerequisite for autonomy and independence, which promotes self-reliance and self-esteem.16 Sensory changes characteristic of ageing, as well as cognitive changes and short-term memory loss, contribute to the difficulty that some people have in knowing where they are, where they want to go, and how to get there. The unpredictable or incomprehensible environment can be confusing for anyone, but it’s especially the case for someone with dementia.
One of the objectives of wayfinding is to enable people to read their environment, which allows them to know where they are and to make appropriate decisions to reach their destination.10
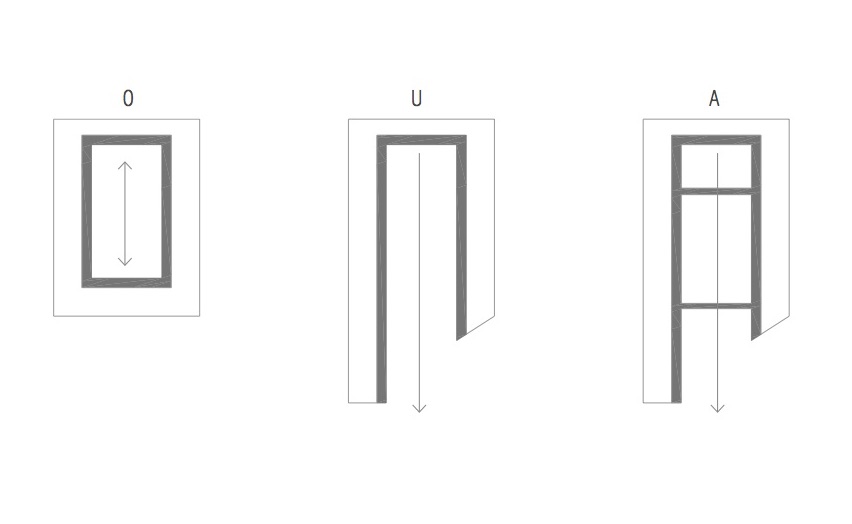
 At the SCUA, the need of residents to be able to walk freely through the house was very clearly observed. Some residents became very angry and anxious when some doors were closed and they couldn’t continue their way. The need to create a path of continuous wandering is an initial concern of the project, and has an influence on the shape of the building itself. While an O form allows a continuous path, it’s closed in itself; and a U allows direct contact with the exterior but not continuous wandering. An A-shaped body, however, with two bridges that cross, helps reduce distances, allowing a continuous walking path and, at the same time, opening towards nature – an important benefit for Alzheimer’s patients (Figure 1). The attempt to go against the continuous corridors with doors on both sides is also facilitated with this formal organisation.
At the SCUA, the need of residents to be able to walk freely through the house was very clearly observed. Some residents became very angry and anxious when some doors were closed and they couldn’t continue their way. The need to create a path of continuous wandering is an initial concern of the project, and has an influence on the shape of the building itself. While an O form allows a continuous path, it’s closed in itself; and a U allows direct contact with the exterior but not continuous wandering. An A-shaped body, however, with two bridges that cross, helps reduce distances, allowing a continuous walking path and, at the same time, opening towards nature – an important benefit for Alzheimer’s patients (Figure 1). The attempt to go against the continuous corridors with doors on both sides is also facilitated with this formal organisation.
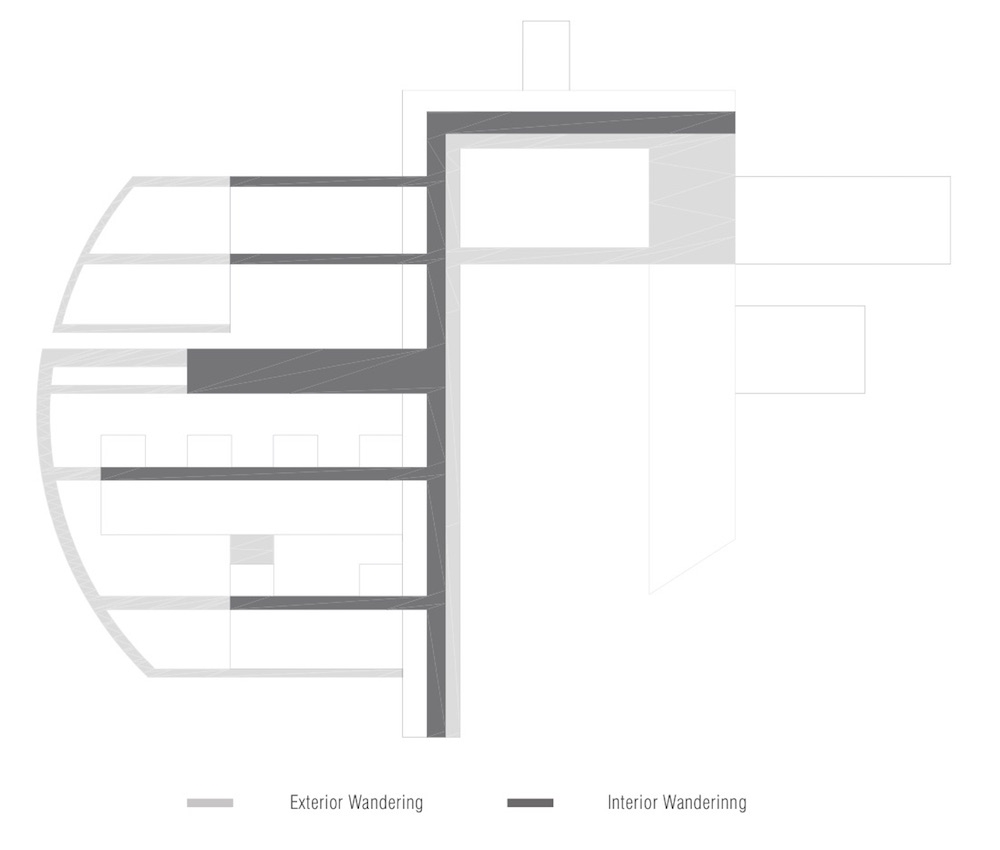
Two safe and quite wide walking paths should be designed – one inside and the other outside, allowing for a continuous walk and with diverse experiences along the way, regardless of the season of the year. In Figure 2, we see a possible A-shaped body with several “arms” that contain the main activities. This configuration allows the creation of interesting and stimulating paths, which extend the interior spaces to a safe and recognisable exterior (Figure 2).
In order to avoid repetitive routes, it could also be interesting to vary the distance between the columns according to the space – if it’s an entrance in a different household, a nucleus, or simply the circulation – thereby giving meaning and dynamism to the space and creating different vibrations along the way (Figure 3).
Trees and living spaces function as reference elements and decision-making points. The School of Education in Setúbal (Portugal), by the architect Siza Vieira, is an example of the use of the tree as an element of reference from which the whole project is developed. In the Herman Hertzberger project for the De Drie Hoven nursing home, the living space that was created at the entrance of each room also works by helping in the making of decisions. The corridor extends and, with places to sit along with a memory-box, reminds the resident of the location of their room. The door of the room needs to have a personally meaningful and recognisable element added so it stands out visually from its neighbours.14
 Promoting the appropriate environment for stimulation and challenge
Promoting the appropriate environment for stimulation and challenge
Herman Hertzberger discusses the importance of creating incentives so that there is still room for each person to appropriate space in their own way.17
The capacity of personalisation, characterisation and transformation of the environment where we live confers a sense of belonging and gives meaning to the existence of each one.10 The opportunity to bring their own furniture and make decisions about the decoration of the room, for example, allows the resident to have an active participation and an opportunity to feel in control in a recognisable and calm environment.
At Peter Rosegger’s project in the nursing home in Graz, Austria, the raised beds work as handrails and, at the same time, as an adapted planting space (Figure 4). Furthermore, in community gardens, raised beds are dividers of space and an incentive to engage in planting and gardening. 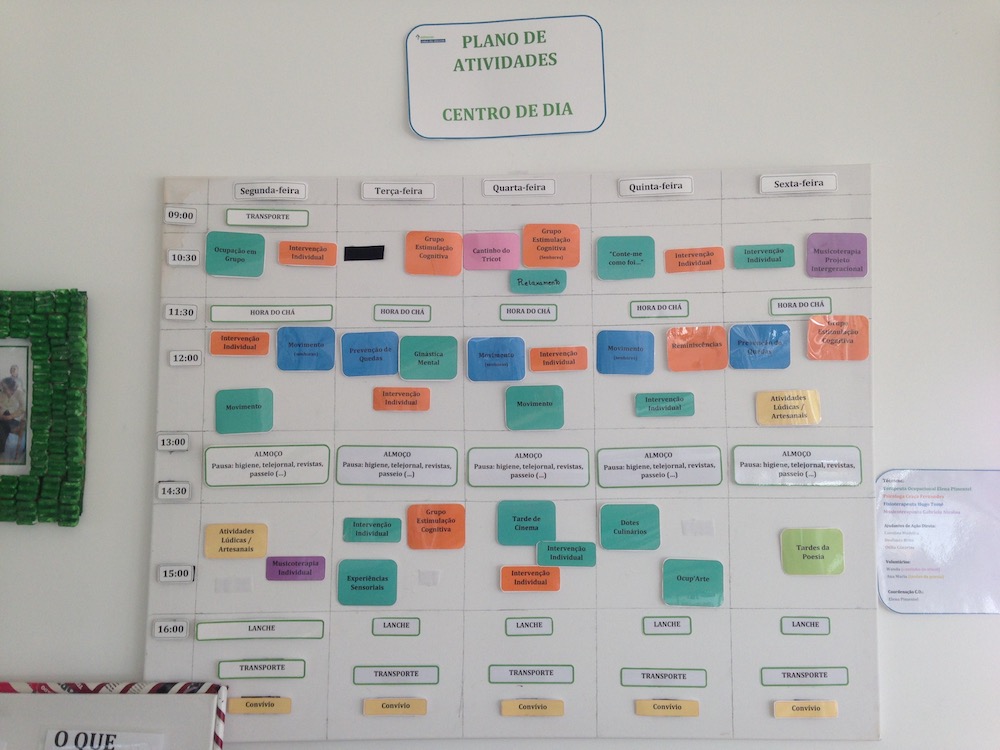
Designing spaces and places that accommodate different levels of activity and types of stimulation, and that vary in size, scale and views, gives people choices about where and how they want to spend their time.14
Support functional capacities through meaningful activities
Each resident must define for themselves what makes sense. Appropriate therapeutic programmes can help support their capabilities that have not yet been lost and prevent other difficulties that may occur during the disease.10
One of the most significant and positive changes in healthcare design was in the area of activity programming (Figure 5). The use of activity spaces has evolved from a large common space to a variety of smaller spaces. These smaller spaces allow residential scale to be maintained while stimulation and noise are more easily controlled.10,11
Each household must contain rooms for therapeutic activities, such as music therapy, plastic arts and occupational therapy. The day centre should also contain spaces for creative activities, a computer room, a library, a cinema, a therapeutic kitchen, a room for occupational therapy, and a therapeutic terrace.
A garden room, a gymnasium and a spa also aim to promote meaningful activities, stimulate the appropriate participation in different interests, and encourage movement.
Promoting contact with the outside
The first study on the influence of architecture on wellbeing and cure of a particular pathology was conducted by Roger Ulrich in his 1984 paper ‘View through a window may influence recovery from surgery’.5 The relationship with the outside is highlighted as indispensable in environments that promote health, and is related to the reduction of agitation and stress in patients with dementia. For these people, the space where they live is often limited to the building and its surroundings. As a result, the exterior space surrounding the building has a special meaning.11 The view to the outdoors allows the patient to be attuned to the days and seasons of the year, the synchronisation of circadian rhythms through light, while it also stimulates the production of serotonin that improves mood and attention.
 While people in an intermediate and final phase of dementia respond to a calm and quiet environment, many residents in an initial phase prefer more active and stimulating environments.
While people in an intermediate and final phase of dementia respond to a calm and quiet environment, many residents in an initial phase prefer more active and stimulating environments.
Access to outdoor spaces is supported by their location in the building. Opportunities that sit distant from the building, the existence of ramps, paths, raised garden beds, shelter from the rain and the sun, and the structure of the garden also encourage this displacement. Roads must be wide enough for a companion to be present, as well as to accommodate wheelchairs. At the same time, they should be circular or enable an easy return to the beginning of the route (Figure 6).
 Many activities can be designed to stimulate long-term memory, such as mowing the lawn, picking up leaves, gardening, or hanging clothes on a rope. Gardening practices describe various aspects of social identity by promoting a sense of community and being an opportunity to socialise. While doing gardening activities with the residents at the SCUA, it was possible to see the joy and freedom felt not only by the residents but also by the carers, who could easily reach and talk to them during this activity.
Many activities can be designed to stimulate long-term memory, such as mowing the lawn, picking up leaves, gardening, or hanging clothes on a rope. Gardening practices describe various aspects of social identity by promoting a sense of community and being an opportunity to socialise. While doing gardening activities with the residents at the SCUA, it was possible to see the joy and freedom felt not only by the residents but also by the carers, who could easily reach and talk to them during this activity.
Sensory stimulation is also very important for people with dementia, and it can be achieved through the use of water (movement and sound) and different plantings.10 The plantation scheme, contributes to the correct stimulation. Each group of plants must respond to a specific characteristic – for example, plants associated with the past that evoke memories; sensory plants that appeal to touch, smell or hearing; and/or plants with medicinal properties.
The power of nature is also evident in the ability to bring the outside into the inside and vice-versa. The existing window in the Fisher House project in Pennsylvania by Louis Kahn (Figure 7) presents, in itself, the opportunity to sit and observe the exterior and, at the same time, the possibility of leaving. Furthermore, in the De Overloop nursing home project by Hertzberger, the existence of a covered area in the front door allows for bringing the interior to the exterior. It also seeks to create a space for family members to gather outside, maintaining privacy, and not confining all the interaction to the interior space of the room. Proposing a place to sit that starts inside and continues to the exterior is a good way to combine these two solutions. 
Develop positive social activities
“Fear of space often goes with fear of solitude”18
The social lives of the elderly can also make a difference to their health and wellbeing. By encouraging residents to interact with their neighbours and by developing a project that seeks ways to serve the community, promotes social contact, and decreases their sense of isolation.
Informal seating spaces promote co-existence and function as places to stop and contemplate (Figure 8). 
The entrance doors in the rooms provide privacy for residents and, at the same time, allows residents to be in contact with the outside, so they can choose between an active and passive interaction. In spite of being safe at home, they have conversations with people who pass by (Figure 9).
The transparent wall of the activity spaces allows the activity that is being developed to be viewed from the outside, encouraging participation without imposing it.
The existence of a chapel and adjacent area for the gathering and practising of religious activities, such as catechesis, preparation of the mass, and conversations about faith, works as an incentive to socialisation through an activity well known and lived by the residents.
Public spaces also allow for greater contact between generations and co-existence outside the units that recalls a normal and healthy lifestyle.10,11
In order to provide good social interaction, it’s also important to provide spaces where people can be alone. As the disease progresses, reading and writing become very challenging activities that require silence and concentration. By talking with people in the initial phase of the disease, it was possible to understand their need for spaces where they could be by themselves, and away from all the noise of public rooms so they could read their books.
Encourage family participation and provide special spaces for carers and health professionals
It’s important to promote living spaces that allow the resident to leave their household properly and move to another space with their family. For more independent residents, spaces such as the cafeteria, exhibition room, playground, public lake, and community gardens are also places of refuge, remoteness and distraction, which are conducive to living with friends and family.
All environments for people with dementia should also have meaningful spaces for employees and carers. Caring for people with dementia is quite demanding and tiring, and carers, no matter how dedicated, occasionally need a break. This place should be designed to provide a quiet and relaxing space, and be a work area. Places to sit, outdoor spaces, a space where private conversations can take place without interruption, all encourage decompression and socialisation. The possibility of the temporary access of these people to a private space can increase their quality of life and, consequently, the care provided.10
Create a familiar environment by stimulating memories
“Can I really, as an architect, draw an architectural atmosphere, this unique density and environment, this sense of reality, wellbeing, harmony and beauty?”19
In addition to all of its architectural potentialities, memory is also one of the human capacities most affected by Alzheimer’s disease. As the disease progresses, memories can be restricted to those experienced at the time. Then, architecture has a greater responsibility to be able to transmit the desired atmosphere and stimulate memories associated with each space.
Emotions, good and bad, are related to a place, which can evoke a series of feelings when revisiting it. Places where you experience wellbeing, comfort, security and privacy are stored in your memory, as are places associated with discomfort, disorientation and insecurity.1
 To create a refuge and place of comfort and intimacy, adaptable to the changing needs of those with Alzheimer’s disease, requires that memories and good experiences are emphasised for people who have limited capacity for memory, while those who still retain some memories have sufficient freedom to appropriate their space as they desire.
To create a refuge and place of comfort and intimacy, adaptable to the changing needs of those with Alzheimer’s disease, requires that memories and good experiences are emphasised for people who have limited capacity for memory, while those who still retain some memories have sufficient freedom to appropriate their space as they desire.
When one reflects on “feeling at home”, the relation that one has with their own house is almost immediate. Our house is present in our memory, often as the most comfortable and intimate place we know. It’s a refuge and our corner of the world.20 This familiar atmosphere can be achieved by assigning characteristics of the spaces of a house to the different spaces of a unit in order to stimulate different memories associated with spaces where one experiences security, comfort and intimacy. 
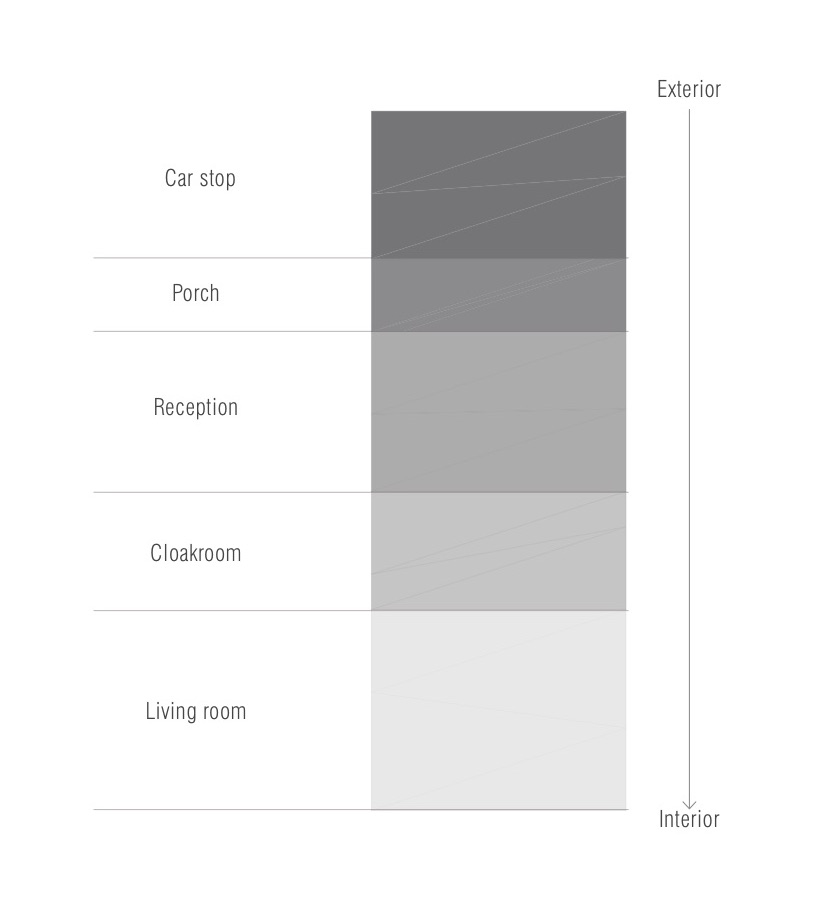
Entry: The entrance is the first impression and difficult to change. It should be warm, friendly and an invitation to all. For residents with dementia, it should serve as a transitional space to lessen confusion and disorientation.10 According to Victor Regnier, creating a memorable first impression involves a change in the spatial hierarchy while entering the building. The stair, which connects the second to the first floor, contributes to a welcoming, explanatory and stimulating entry that contributes to the residential appearance.11 The entrance should then be divided into small spaces, with the aim of achieving a more intimate and familiar environment, and not confronting the residents with the size of the unit (Figure 10). 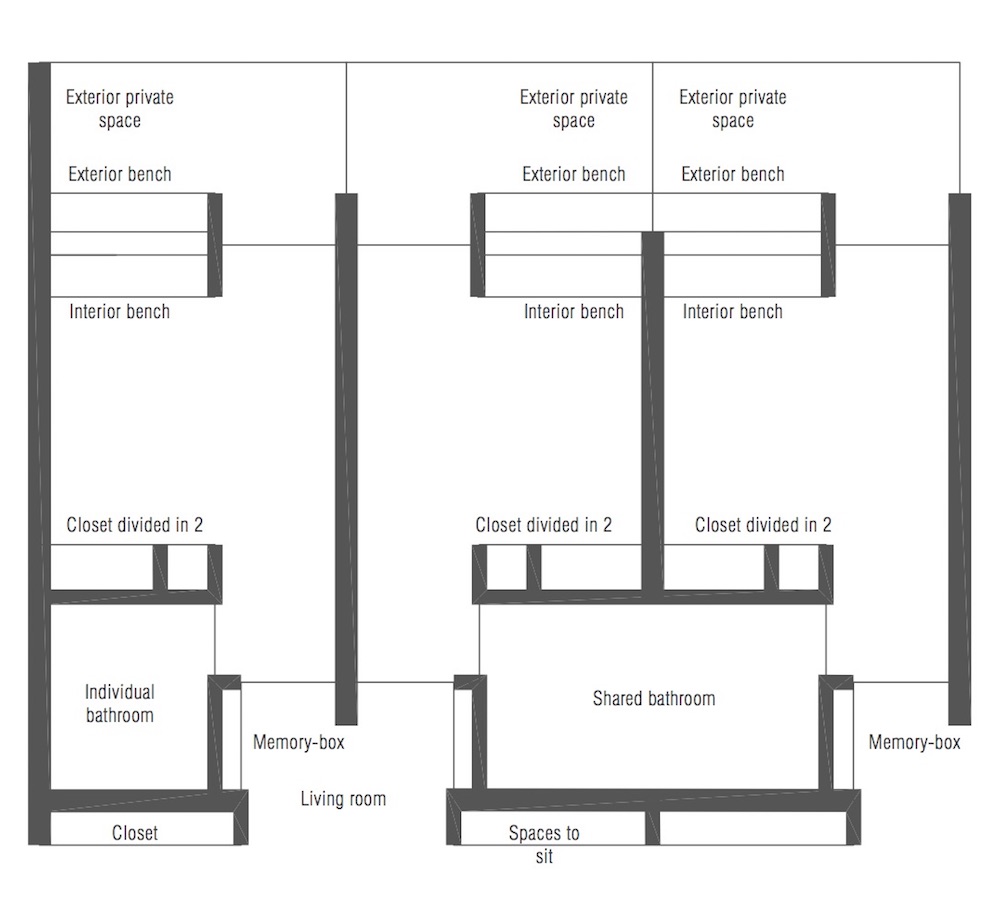
Living room and dining room: In a special unit for Alzheimer’s patients, living rooms should be divided into smaller spaces. Using a library, a room to watch television, and other special spaces ensures that the group stays small and that space is used.10 For many people, mealtime is the most anticipated moment of the day but, if the environment doesn’t lead to socialisation, this experience may not be pleasant. By dividing residents in households, several living and dining spaces are created where these activities can be performed as a family. However, there must also be a large dining room, where users of the day centre have their meals and more autonomous residents from the nursing home can join. These social areas are spaces filled with windows and plenty of natural light, and are conducive to drinking a tea or coffee, reading, receiving visitors, or just sitting back and enjoying the light.
Kitchen: A kitchen is a very familiar space that individuals recognise and know what types of activities are appropriate for that space. Despite not having the objective of preparing regular meals, small-scale kitchens must be designed to provide therapeutic activities with meaning and experiences for people with dementia. A safe and accessible kitchen also facilitates group activities, such as cooking and decorating cookies, making ice cream or washing vegetables.
Rooms: The design of the room has a great influence on the patient’s wellbeing.21 Instead of projecting rooms with as little space as possible, we should expand thinking and design rooms that are spacious enough to encourage a normal lifestyle.
Discussion about the advantages and disadvantages of private versus shared rooms doesn’t define clearly which is best, since there are pros and cons for both solutions. Based on the experience at the SCUA, by observing residents and talking with carers, seeking to improve the quality of sleep, privacy, and facilitate the work of those who perform the night shifts and hygiene care daily, the option of individual rooms with a shared bathroom is seen as positive because it encourages personalisation and individualisation of care (Figure 11). Each resident has their own clearly defined space with a window, wardrobe and equal access to the front door and bathroom, contributing to better privacy and, at the same time, supporting the carers in maintaining control easily.14
 Duplicating the existing furniture configuration in the home room can make the environment more familiar and help confused residents feel more comfortable in their new environment. When surrounded by personal clues and memories of the past, their achievements and social roles, people with dementia can identify where they are. With this notion of self, residents feel more in control and express themselves in a more positive way (Figure 12).22
Duplicating the existing furniture configuration in the home room can make the environment more familiar and help confused residents feel more comfortable in their new environment. When surrounded by personal clues and memories of the past, their achievements and social roles, people with dementia can identify where they are. With this notion of self, residents feel more in control and express themselves in a more positive way (Figure 12).22
Lighting and colour
To achieve a familiar atmosphere, one of the most fundamental details in the project is light. It’s important, especially in long-term care institutions, to incorporate as much natural light as possible in all spaces and seek a balance with artificial light.
It’s necessary to bear in mind that residents with dementia in special care units are not able to physically modify their environment to avoid brightness or improve lighting conditions to meet their needs. This can lead to a series of problems, such as anxiety, confusion and anger.10
Alvar Aalto, in Paimio Sanatorium (1932) (Figure 13), was greatly concerned with the entrance of light, the quality and regeneration of the air, contact with the sun, and hygiene, mainly in relation to the original users of the project: patients with Tuberculosis.23 Aalto was concerned for the patient as “the horizontal human being”. As the majority of their time was spent lying down, the patient must be involved in an architecture conscious of his situation and, for this reason, it’s necessary to take into account questions of colour, light entrance, heat, sound, etc. 
Several researchers have shown that exposure to light can reduce agitated behaviour and improve sleep cycles in people with Alzheimer’s at an advanced stage.10 Light also reduces a symptom in Alzheimer’s disease called sundowning, which results in a feeling of confusion and agitation at sunset. At the SCUA, it was possible to have conversations with residents who said the best part of their day was when the sunlight entered directly in the living room and touched their face.
Colour is also an element of great importance. For Alzheimer’s patients, it gains greater importance by allowing the identification of spaces and contrasting surfaces.
In the Sanatorium of Paimio, colour is used as an identifying element of space, making it a reference and a prominent place (Figure 14).
 The results of a study indicate that yellow and red are easier colours to identify for these patients than blue and green, and patients in a more advanced stage of the disease have a greater difficulty in distinguishing mixed colours.24 In Figure 15, we can see the use of colour as a way to identify different areas and help in decision-making (Figure 15).
The results of a study indicate that yellow and red are easier colours to identify for these patients than blue and green, and patients in a more advanced stage of the disease have a greater difficulty in distinguishing mixed colours.24 In Figure 15, we can see the use of colour as a way to identify different areas and help in decision-making (Figure 15).
Religion and spirituality
Religion and spirituality positively affect each person’s life and can have a great positive effect when introduced as part of a therapy. Many doctors believe that medical interventions can be more effective when reconciled with the spiritual activities of patients.25
The existence of a chapel in an Alzheimer’s facility – as an element that is different from the whole unit by breaking with regularity and materiality – is, in itself, an opportunity to create a reference place where people can go and remember a normal life (Figure 16). Often the only way to interact with residents is through religion and religious symbols. The chapel seeks to be a place of refuge, contemplation and meeting between residents and neighbours, where everyone feels welcomed, comfortable and safe. 
Conclusions
Architecture is often reduced to its technical components to solve objective problems, understood only by professionals, and applied without any attempt to accept the realities of their time. In order to humanise architecture, we need to take into account the real needs of the future user of the space.
Alzheimer’s patients are very sensitive to the physical environment in which they live and the atmosphere they feel. Many physical characteristics of the architectural space can therefore contribute to a better experience for those with the disease and to a reduction in anxiety and agitation.
The opportunity to visit and learn about the reality lived in a special care unit was, without doubt, very enriching. Through contact with patients, asking questions, listening to stories, and observing the lives of all the people involved, it was possible to really learn about the difficulties of Alzheimer’s disease for patients, relatives and carers, and to see the importance of an experience like this at the beginning of an architecture project.
This study seeks to raise awareness about the need for preliminary research before embarking on any architecture project, and for the human capacities of architecture, by relating architectural characteristics with the physical, cognitive and emotional needs of people.
Author
Catarina Oom is an architect at Pinearq, in Barcelona, Spain.
References
- Stenberg, E. Healing Spaces: The Science of Place and WellBeing. (1st ed). USA: Belknap Press; 2009.
- Huelat, JB. Healthcare Design Magazine [Internet]. The healing experience. 2009. Available from: https://www.healthcaredesignmagazine.com/trends/architecture/healing-experience/
- Hamilton, K. Congress: Architecture and Health in Dialogue. Lisbon; 2015.
- Brawley, E. Environmental design for Alzheimer’s disease: a quality of life issue. Aging Ment Health. 2001; 79–83.
- Ulrich, R. View through a window may influence recovery from surgery. Science. 1984; 224:420–1.
- Walk, D, and Dickerson, B. Clinical features and diagnosis of Alzheimer’s disease. Up to Date; 2015.
- View, W. How the spaces we shape shape us: the impact of the built environment on memory care; 2015.
- WHO. Dementia: number of people affected to triple in next 30 years; 2017.
- Marquardt, G, Bueter, K, and Motzek, T. Impact of the design of the built environment on people with dementia: an evidence-based review. Heal Environ Res Des J. 2014; 8:127–57.
- Brawley, E. Designing for Alzheimer’s Disease: Strategies for Creating Better Care Environments. 1st ed. New York: John Wiley & Sons; 1997.
- Regnier, V. Design for Assisted Living: Guidelines for Housing the Physically and Mentally Frail. New York: John Wiley & Sons; 2002.
- Chmielewski, E, and Eastman, P. Excellence in design: optimal living space for people with Alzheimer’s disease and related dementias; 2014.
- Henry, R. Healthcare Design Magazine [Internet]. A clear path: addressing changes in patients’ mobility requirements; 2017. Available from: https://www.healthcaredesignmagazine.com/trends/research-theory/a-clear-path/
- Calkins, M. Supportive and therapeutic environments for people living with dementia. Gerontol Soc Am. 2017; 58.
- Matambanadzi, S. Healthcare Design Magazine [Internet]. EFA 2013: Designing for daily life with dementia; 2013. Available from: https://www.healthcaredesignmagazine.com/architecture/efa-2013-designing-daily-life-dementia/
- Marquardt, G. Wayfinding for people with dementia: a review of the role of architectural design. Heal Environ Res Des J. 2011; 4:75–90.
- Hertzberger, H. Lessons for Students in Architecture. (5th ed). Rotterdam: 010 Publishers; 2005.
- Tuan Y-F. Space and Place: The Perspective of Experience. (8th ed). Minneapolis: University of Minnesota Press; 2001.
- Zumthor, P. Pensar a Arquitetura. (7th ed). São Paulo: Gustavo Gili; 2005.
- Bachelard, G. A Poética do Espaço. (1st ed). São Paulo: Martins Fontes; 1996.
- Dreher. M. Hospital room design and health outcomes of the aging adult. Heal Environ Res Des J. 2011; 4:23–36.
- Zeisel, J. Improving person-centered care through effective design. J Am Soc Aging. 2013; 37:45–52.
- Norri, MR. Alvar Aalto em Sete Edifícios. 1999.
- Wijk, H, Berg, S, Sivik, L, and Steen, B. Colour discrimination, colour naming and colour preferences among individuals with Alzheimer’s disease. Int J Geriatr Psychiatry. 1999; 14.
- Brawley, E. Design Innovations for Aging and Alzheimer’s: Creating Caring Environments. (1st ed). New Jersey: John Wiley & Sons; 2006.
Organisations involved