Healthcare / Sustainability
Food as medicine, farm as therapy: a multidisciplinary approach to planning a food-based social enterprise for Toronto Rehabilitation Institute
By Adeline Cohen, Ryan Turnbull, Kendra Delicaet, Edward Rubinstein, Megan Torza, Phil Mount, Kathleen Camaya and Brenda Nistor | 05 Sep 2018 | 0
This research project explores the design and business model of an urban farm that aims to be financially self-sufficient while providing a variety of health benefits for patients, including therapeutic recreation, occupational therapy, improved mental health, and increased food literacy.
Authors of scientific paper:

Abstract
The Toronto Rehab Urban Farm (TRUF) social enterprise is inspired by the transformation of hospital food environments to foster healthy behaviours, and by the changing philanthropic landscape in Canada as non-profit organisations move beyond traditional revenue sources to integrating earned revenue. The 18-month feasibility study and business planning process involved patients, clinical and administrative staff of University Health Network (UHN) in co-creating a social enterprise that is financially independent of hospital funding while creating opportunities for patients to engage in therapeutic gardening and cooking programmes.
Social enterprise business planning involves both demonstrating financial viability and assessing social impact. To define project scope, a literature review assessed current evidence, while 17 semi-directed, qualitative, 30-minute interviews captured the patient perspective. The staff perspective was captured in six preliminary semi-directed, qualitative interviews of 45 to 60 minutes, a quantitative survey with 124 participants during the feasibility phase, as well as 26 semi-structured qualitative interviews of 45 to 60 minutes during the planning phase. Operational needs and revenue projection were evaluated through market analysis and an environmental scan of 62 farms, including 31 Canadian farms, 26 in the US, and six farms in other countries. A subset of 18 farms was selected as comparators for further estimating operational needs. Finally, multiple stakeholders were engaged through ad hoc meetings, as well as a co-design workshop to visualise the collaboration between UHN stakeholders and the independent farm operator.
The social enterprise was modelled as a partnership between two legal entities: UHN and an independent commercial farm that has yet to be selected. TRUF will improve patient transition into home and community care by supporting research and therapeutic programmes aimed at improving physical and mental health. This social enterprise will foster healthy eating behaviour and develop food literacy and cooking skills of patients currently involved in spinal cord, cardiac and neurological programmes. The farm infrastructure will be separated between commercial and programming infrastructure. A permaculture garden and a patient-use greenhouse will be used to engage in learning and therapeutic programmes, and to supply a sizeable portion of the ingredients needed in cooking programmes for the hospital. A not-for-profit or private partner sharing UHN’s values would operate a climate-controlled greenhouse equipped with a vertical hydroponic growing system, a seed-starting and micro-green operation, and a rooftop garden for onsite and external sales.
After applying corrective measures, the conservative estimated sales for years one, two and three were CA$203,000, $240,000 and $240,000 respectively, with the vertical farming production accounting for 84 per cent of revenue. Annual expenses related to food production were projected at $212,000, with human resources and utility costs accounting for 79 per cent of the expenses. On the programming side, the operating expenses included utility, maintenance and security costs of $30,000 a year, and supplies needed to run the co-designed patient programmes are estimated to be about $4000 a year. UHN would substantially benefit from the partnership thanks to an increased capacity for research and programmes.
Fundraising for the initial capital expenditure is a key contributor to the social enterprise viability, since an initial capital outlay of about $4.4 million would be required if the project moves forward.
Overall, the social enterprise can be considered highly cost-efficient from an operational perspective. Over time, the farm operation has the capacity to generate a small profit that can be reinvested in furthering the partnership’s social mission. TRUF social enterprise is not only achievable but also replicable in many hospital and care facilities endowed with sufficient land.
Keywords
Introduction
The healthcare system is constantly changing, both adapting to innovations in research as well as responding to the many healthcare cost drivers. Given that increases in healthcare funding don’t meet the financial needs of hospitals, economies of scale need to be identified. A consistent cost-saving strategy in Canadian hospitals has provided a strong motive to outsource the provision of food to external service providers, thereby relinquishing control over foods offered to staff, patients and their families. Today, unhealthy foods, which contribute to diet-related chronic diseases, are widely available in public settings across Canada, and many Canadian health and scientific organisations recommend improving the food environment in such institutions.1
Both direct and indirect health expenses for patients with diet-related chronic diseases cost the Canadian healthcare system $26 billion annually.2 The most recent Canadian nutrition data suggests that there has been little improvement in dietary habits over the past 10 years, and the overall quality of the Canadian diet is poor.3 Improving the food environment is increasingly seen as a key lever to support healthy eating behaviour.4 In fact, promoting healthier food environments in public settings may help mitigate adverse health outcomes.5
There is growing evidence that supports combining nutritional education with hands-on, skill-building cooking activities. Although the literature is limited, researchers have begun to assess the effects of cooking activities in nutrition education programmes, and they’ve found preliminary evidence indicating that increased cooking knowledge, skills and behaviour can help improve fruit and vegetable consumption.6
Outside healthcare, many non-profit organisations are working to change the food environment by developing innovative solutions that increase the availability of and access to healthy food for communities, focusing in part on the most vulnerable and food-insecure populations. The rise of community food centres in Canada is seen as a means of increasing food access and equity, reducing social isolation, and improving health and food skills.7
Further, the charitable sector in Canada is increasingly turning to ‘earned income strategies’ in order to finance their important community impact and mission-driven work. The rising tide of social enterprises in Canada has been stimulated by ever-increasing austerity with governments dolling out less in grants than ever before.
Another contributing factor is the almost complete eradication of core funding for the charitable sector, which has been replaced by project-based funding. The Social Enterprise Sector Survey in Canada found that social enterprises employed 31,000 people and served 5.5 million people through the sale of products and services equalling $846 million in sales. This provides a strong indication that the social enterprise movement is strong and growing in Canada, and making a substantial contribution to the economy.8 A significant number of the social enterprises in Canada operate in the food and agriculture industry, as a result of the pressing challenges that are escalating in our food system, such as the rise of food insecurity and dietary-related chronic disease.
An opportunity for Toronto Rehabilitation Institute
The Toronto Rehabilitation Institute (TRI, or Toronto Rehab) is a member of the University Health Network (UHN), a group of research hospitals affiliated with the University of Toronto. Toronto Rehab’s mission is to develop solutions for people living with the consequences of illness, injury and ageing through excellence, innovation and the integration of discovery, education and care. Strategic directions to 2021 include optimising patients’ safe integration back into the community, and integrating education and research into each patient care experience.9 TRI is comprised of four campuses, two of which – Lyndhurst Center and the adjacent Rumsey Center – are the potential sites for the development of a food-based social enterprise. These two sites in north Toronto host three rehabilitation programmes for people recovering from spinal cord injuries, cardiac events, and neurological injuries and illnesses.
In 2014, UHN’s Department of Energy and Environment undertook a year-long exploration of the food ecosystem to understand how the use of local Ontario food could be developed. The project was launched in response to the Ontario Bill 36, Local Food Act of 2013, which encouraged increased use of local food by public-sector organisations to support local food economies and systems.10 The project engaged patients, hospital staff, visitors and the broader community in crowdsourcing solutions and ideas that could help integrate more local foods within the UHN food ecosystem. A multidisciplinary advisory committee assessed the 109 ideas gathered over a four-month period against various feasibility criteria. The development of an urban farm at Toronto Rehab’s Lyndhurst Center was considered as it not only addressed Bill 36 but it also provided a variety of opportunities for Toronto Rehab to achieve its strategic goals, improve patients’ mental and physical health, ease their transition out of rehab, and improve the food environment of the hospital.
The resurgence of hospital farms
There is growing evidence that “green” exercise11,12 and, specifically, gardening13,14 have important physical and mental health benefits.15 The therapeutic benefits of green spaces for both mental and physical health have been well documented. These include: improvement in mood, memory, cognitive abilities, stress hormones levels and immune functioning regulation, as well as lowered cardiovascular risks.16 Historically, many hospitals grew food on their own land to feed their patients and staff. While most of these on-site farms have been dismantled, a measured resurgence of this approach is taking place across North America.17 Hospitals including the Lankenau Medical Center, St Luke’s University Health Network, Henry Ford West Bloomfield Hospital and the Boston Medical Center make use of hospital land and building rooftops to grow organic produce that can be used for hands-on cooking classes, hospital cafeteria food or to stock food pantries servicing food-insecure patients.
Many of these projects depend on philanthropic support or hospital funding to operate. In the case of Toronto Rehab, stakeholders looking into the development of an urban farm decided early on that the project needed to be financially self-sufficient in order to remain immune to fluctuations in healthcare funding.
This paper discusses the process and outcomes of involving various healthcare leaders in the development a food-based social enterprise on hospital land that is financially independent of hospital funding while offering multiple social and health benefits. The social enterprise is referenced throughout this paper as Toronto Rehab Urban Farm or TRUF. It’s composed of the production of leafy greens, microgreens and herbs for commercial purpose, combined with the delivery of food-based patient therapy, involving both gardening and cooking. The social enterprise is composed of two independent but co-ordinated legal entities, a farm operator and TRI, forming a close-working partnership to deliver social, health and financial outcomes.
Methodology
The 18-month long feasibility study and business-planning project incorporated various tools borrowed from service design and business planning methodologies, as well as the completion of a literature review of relevant evidence. Social enterprise business planning not only assesses and plans a business but also identifies how the operation can meet social and/or environmental objectives. In the case of TRUF, health and social gains were prioritised and explored.
Analysis of impact
A total of 17 semi-directed, qualitative, 30-minute interviews were conducted with patients from Lyndhurst and Rumsey Centers to understand patients’ interest in gardening and cooking programmes, their accessibility needs, and their intention to both participate in therapeutic activities and purchase food. The perspectives of TRI staff were captured through six preliminary, semi-directed, qualitative interviews of 45 to 60 minutes and a quantitative survey with 124 participants (29 per cent of the staff population of TRI Lyndhurst and Rumsey Centers) during the feasibility phase, as well as 26 semi-structured qualitative interviews of 45 to 60 minutes during the planning phase. Staff offered their opinions on the social enterprise concept, how the urban farm could further their therapeutic or research efforts, how programmes could be implemented, and what measurable social and health outcomes could result from patient interaction with the farm. The survey also explored staff’s intention to purchase farm produce and their preferred point-of-sale settings.
Analysis of business operations
An environmental scan exploring the current urban and vertical farm landscape was undertaken to understand the market and similar business models. Of special interest were farms located in Toronto and other urban areas in Canada and the United States (US) – programmes that included a greenhouse as part of their infrastructure or used innovative techniques that maximised growing surfaces, such as vertical or rooftop farming.
We collected information from 63 farms to better understand characteristics such as farm size, infrastructure, staffing models, production size, and clientele. The study looked at 31 Canadian farms, 26 in the US and six in other countries. The diversity of this sample was sought to ensure relevant information was included in the plan. The data found through Internet searches and review of media was complemented by 23 semi-structured interviews of 45-60 minutes with farm managers and urban farming experts, including nine for which farm visits were also conducted. From this sample of 63 farms, 18 were selected to constitute a comparator subset, as they were similar in land surface (below 0.2 acres) and infrastructure (greenhouse or rooftop). This subset helped anticipate the TRUF potential production volume and its operational needs. A second series of six semi-structured interviews of 45 minutes was conducted with Toronto urban farm operators with the purpose of collecting feedback on early assumptions regarding TRUF operations, marketing strategy, and the partnership agreement that would be needed between the farm operator and TRI.
The urban farming market was further assessed through a review of current literature. Of particular interest was data related to local food consumption and three potential sales channels: farmer’s markets, community supported agriculture (CSA), and restaurants or food services.
Leadership engagement and co-design
The TRUF project can be considered as ‘from the middle out’, as opposed to taking a ‘top-down’ or ‘bottom-up’ approach to programming and infrastructural change. UHN’s Department of Energy and Environment initiated the project with financial support from the Ontario Greenbelt Fund. For the project’s planning phase, administrative responsibilities were passed to OpenLab, a design incubator housed at UHN, and the project co-ordination was supported by the Toronto Rehab Foundation and the Ben and Hilda Katz Family Foundation. Another key funder was the McConnell Family Foundation’s Innoweave programme – a social innovation initiative that supports intra-preneurship within organisations by funding the coaching services of a social enterprise consultant.
Key stakeholders from across UHN and TRI were engaged throughout the feasibility and business planning processes. These included senior leaders and key informants, who were selected for their complementary knowledge of UHN programmes, practices and facilities, as well as patient partners who provided their lived experience of the cardiac and spinal cord rehab programmes. The project governance was provided by a stakeholder committee with an advisory function, and a steering committee with decision-making capacity. The stakeholder committee provided opinions from: former patients; patient care and allied health; facilities and infrastructure; nutrition services; and the Toronto Rehab Foundation. Feedback and buy-in on major directions were sought periodically during six ad hoc meetings. In addition, individual leaders provided access to internal data and connections with informants throughout the UHN network, while they also participated in working group meetings tackling three aspects of the project: infrastructure design, user research, and business model co-design.
As data was being collected, stakeholders helped assess and refine a business model using Osterwalder’s business model canvas,18 determined multiple objectives for TRUF, mapped stakeholders using the Adaptive Leadership Framework,19 and refined a blended value proposition for the farm partnership. Both committees also guided the development 3D rendering of a patient facility, a greenhouse, and outdoor landscaping with DTAH architects, developed several patient journeys representing the potential diverse interaction patients could have with the farm, and established a three-year therapeutic programme plan. A final co-design workshop was held to define how partnership between a farm operator and TRI should be developed to best integrate commercial food production with therapy.
Research limitations
The recruitment of individuals for qualitative interviews was not blinded, and many patients and staff members chose to participate because they were curious or supportive of the urban farm project. While interview questions remained neutral, recruitment may have favoured supportive individuals. Conservative assumptions were used when developing sales predictions and estimating participant numbers for therapeutic programs to account for an eventual biased recruitment.
Another limitation was the inaccessibility of some information that has created two “blind spots” in the analysis. First, the inability to engage in a competitive procurement process limited the access to confidential data about the cost and projected production of vertical farming equipment. Second, it was impossible to engage in developing a partnership with a farm operator without full commitment. These limitations were partially addressed by working with an urban farming consultant who represented the interest of a farm operator in the co-design of the social enterprise model. 
Co-design of a social enterprise
User-centred farm design
The first phase in the development of the business plan was to discuss the assumptions of the feasibility study with patients and staff. As a large majority of patients at Rumsey and Lyndhurst use assistive devices, accessibility and safety were key considerations in the design. A covered path between the two centres was designed to facilitate travel between the two rehabilitation centres, and a greenhouse equipped with a vertical farming system was favoured for their accessibility. Another focus was the importance of mental health and relaxation, and design elements supporting these will be integrated into the design of the greenhouse (eg, natural light, spacious volumes and an abundance of plants). A resting lounge area connected to the Lyndhurst building was also deemed necessary early in the project. The urban farm concept was well received among all users of the site, and encouraged the exploration of features such as the addition of a demonstration kitchen, designed to accommodate 20 people, and a rooftop garden.
For the farm’s design, the space offers multiple opportunities for learning about sustainable and organic farming. The landscape includes a permaculture garden – a system of cultivation intended to maintain permanent agriculture by relying on renewable resources and self-sustaining ecosystem. Additionally, a patient-use greenhouse in part of the commercial greenhouse was included to engage patients in educational and therapeutic programmes, and to supply a sizeable portion of the ingredients needed in cooking programmes. 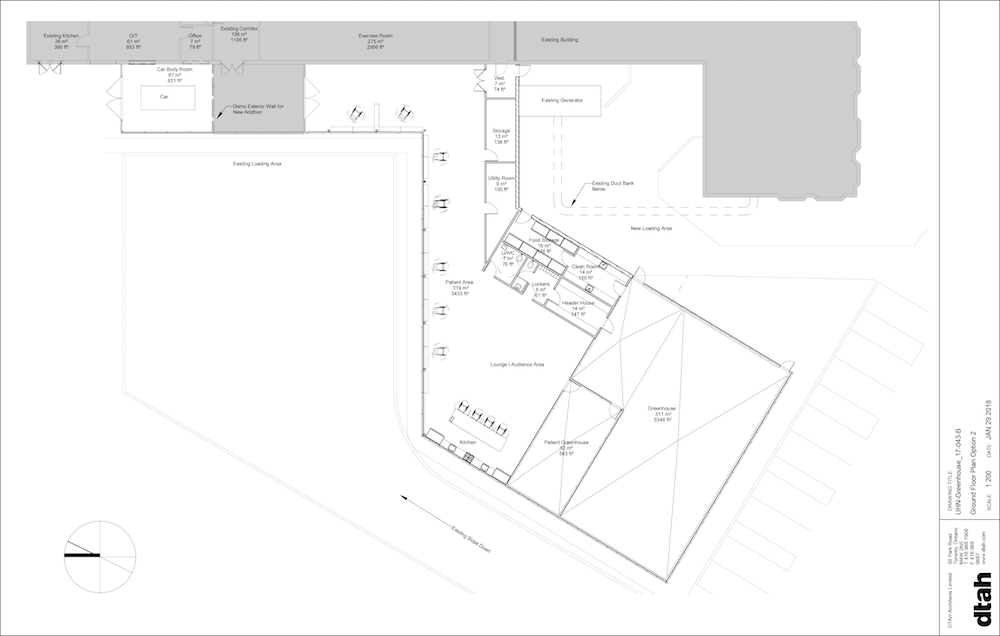
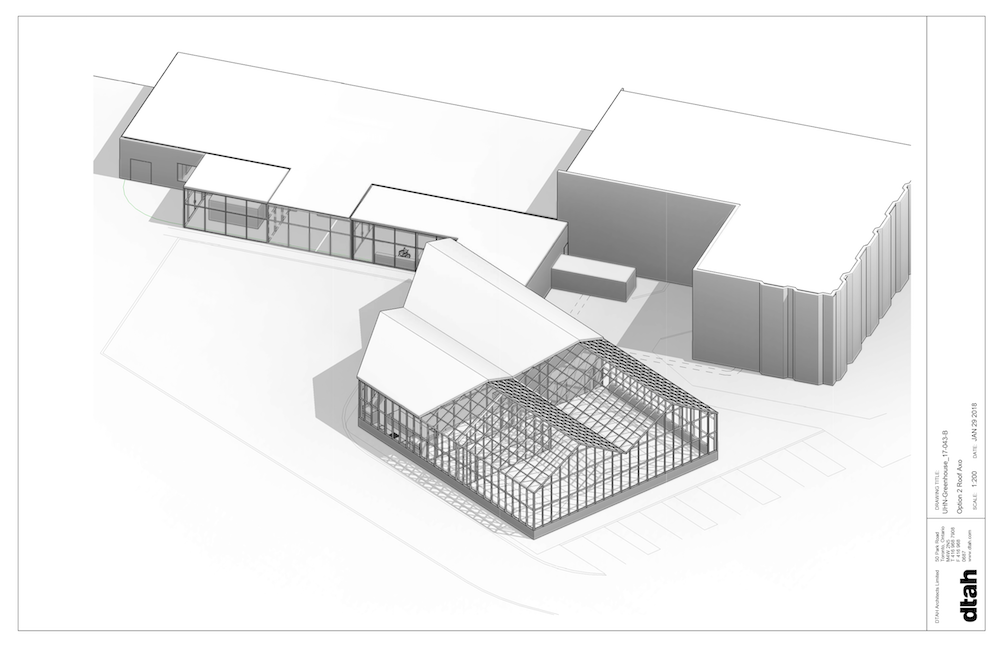
Community spaces were made distinct from the greenhouse and rooftop farm commercial spaces. Overall, the farm is designed to physically separate the two main activities of the farm – food production and therapy – limiting cross contamination and favouring collaboration and cross-benefits. Between the feasibility study and the business plan phases, the project grew to prototype a fully accessible farm, which complemented and supported patients’ rehabilitation, confidence and independence in transitioning into community and home care.
Thinking outside traditional revenue streams
From an early stage it was recognised that in a research hospital environment, where numerous priorities compete for limited funding, operating costs would need to be minimised to ensure the project’s success. To achieve its social mission while ensuring long-term viability, it was agreed that the urban farm would follow a social enterprise model. Its financial model would look beyond traditional revenue sources, such as fundraising and grants, on which the charitable sector often relies. In addition, the project would consider earned revenue through sales of goods and services.
The feasibility study identified a business model that would achieve cost neutrality for TRI. By developing a social enterprise that grows and sells enough food to sustain its operation it could provide free or at-cost services to TRI. About $200,000 a year is required to sustain a reasonable operation. Given the limited size of land available for food production, it was agreed that growing food vertically and choosing fast-growing crops would help meet the production volume required. The production of leafy greens, herbs and micro-greens are currently identified as the primary crops. Hydroponic production was determined to be the most desirable growing mechanism. The feasibility study also brought the early consensus that the farm operator would likely need to sell its produce to a market broader than the TRI sites.
The planning phase refined the expenses and revenues projections, and several sources of revenue channels were further researched. It was confirmed that the commercial farm would benefit from the captive market on site of the rehabilitation centre. Located in an affluent residential area with limited on-site food options, sales would benefit from substantial demand among the 6600 yearly users of the site and its neighbourhood of 3900 households. The rooftop garden was added to increase the variety of produce available for sale. It was also agreed that paid gardening lectures offered by the farm operator could complement the therapeutic programme outside of clinical hours.
Partnership design
A key aspect in the participatory design of the social enterprise model was the development of a partnership model. It was understood early in the process that while the hospital system wasn’t interested in running a farm, they were keen on housing a farm and contributing to its success. This included early agreement that philanthropy would fund the capital and start-up cost of the farm to provide the partner with a significant financial advantage. The TRUF partnership would make use of each partner’s strengths, and roles and responsibilities would be clarified in a service agreement binding the two legal entities together, to achieve complementary objectives of therapy and financial self-sufficiency. UHN, for example, would facilitate access to capital funding through its Toronto Rehab Foundation, and in exchange receive a worry-free therapeutic farm requiring minimal co-ordination. The commercial farm would maintain a safe and organised food production process, monitor a list of tasks available for gardening therapy, and provide free produce for cooking classes in exchange for a captive market for its paid products and services. 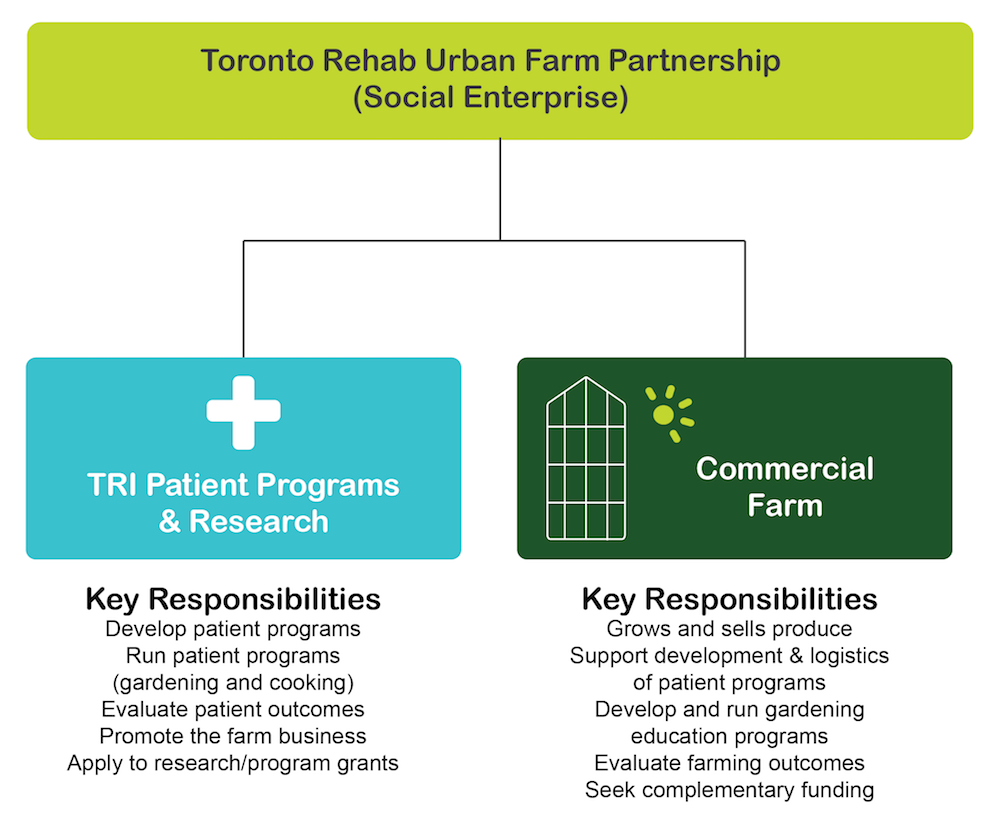
UHN will develop a partnership with a non-profit organisation or private company aligned with the values and vision of TRUF. This partner will have the requisite expertise and a proven track record of being able to run and manage a viable urban farm that incorporates numerous growing methods.
To manage the partnership, key stakeholders will form an advisory committee to assess the model, and make corrective and optimising decisions to strengthen the operation of the TRUF partnership. In particular, the committee will review monitored data about the partnership performance and its achievement of patient outcomes.
Programme design
The process of developing patient programmes involved multiple clinical staff and patient partners. Individuals with lived experience worked with occupational therapists, recreational therapists, clinical dietitians and managers to discuss programmes that are most relevant to the populations attending both rehabilitation centres. A focus was placed on the primary tenants of Lyndhurst Center, inpatients of the spinal cord programme. It was decided that gardening and cooking programmes would expand over a three-year period to include spinal cord outpatient programmes, cardiac rehabilitation programmes, the pain management clinic, and a programme for patients with neurological conditions. Stakeholders also decided that the farm operator was well placed to prepare the material and co-ordinate programming, while clinical staff would be responsible for running therapeutic programmes and for the safety of patients. 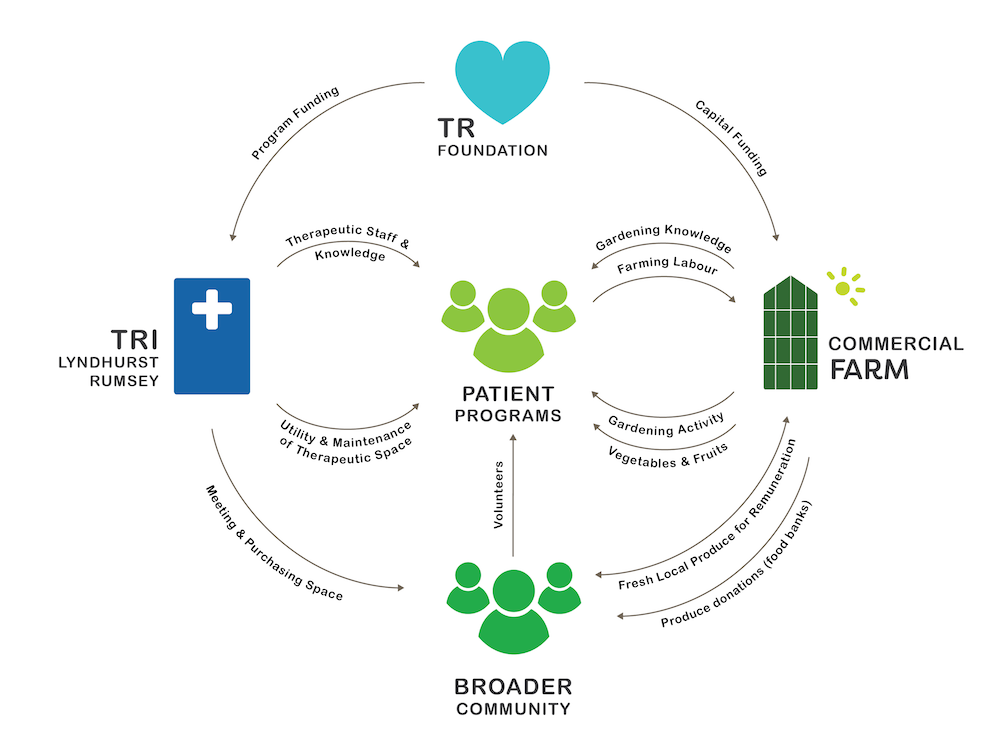
Another important aspect of this phase was identifying the value of outcome-based evaluation. As all clinical staff are used to record patient outcomes, integrating the outcomes of farm participation was considered a simple task that could easily be integrated into current processes. In addition, many clinical staff and researchers pointed out the added benefit that TRUF would provide in expanding research opportunities in both spinal cord and cardiac rehabilitation. Conducting clinical research in a farm environment broadens the range of research funding that can be pursued to further rehabilitation research.
Project viability
Estimating food production in an outdoor space that hasn’t been farmed before can be challenging. Yield can vary based on crop selection, seasonal weather, rainfall, sun exposure, pests/diseases (including animals from the nearby ravine), harvest methods, planting dates, and succession planting schedule. We chose to estimate a revenue range from each growing area rather than relying on a single value. Farming in a controlled environment, such as a climate-controlled greenhouse, is easier to predict. Given the unusual nature of this model, however, we anticipated a learning curve over the first few years, and reduced growth estimations by 30, 20 and 10 per cent for years one, two and three respectively.
After applying corrective measures, the conservative estimated sales from years one, two and three were $203,000, $240,000 and $240,000 respectively, with the greenhouse production accounting for 84 per cent of revenues. Expenses related to food production were projected at $212,000 a year, with human resources and utility costs accounting for 79 per cent of the expenses of the commercial farm.
Operating expenses, consisting of added utility, maintenance and security cost, represented $30,000 a year, and supplies required to run patient programmes cost $4000 per year. After considering the needs of the partnership, it was decided that a fifth of a full-time employee (FTE) cost required to support the patient programmes could be passed on to TRI. This cost would represent about $10,000 a year. TRI would substantially benefit from this partnership since, for a cost of $44,000 per year, TRI would increase its research and programme capacity. The revenue generated from applied research grants was estimated at $600,000 a year, which could cover a large part, if not all, of operating expenses.
To get the urban farm off the ground, significant investment to cover start-up costs need to come from major gifts through a capital fundraising campaign. An initial capital outlay of about $4.4 million dollars is required to build the greenhouse and patient area, renovate the roof, and modify the site landscape.
Conclusion and discussion
Overall, the social enterprise can be considered operationally cost-neutral. The farm operation would break even on the second year and has capacity over time to generate a small profit, which could be re-invested in furthering the partnership’s social mission. The TRUF partnership is not only achievable but it could also be replicated in hospital and healthcare facilities possessing sufficient land.
At the time of writing this paper, a decision to move forward has yet to be made. The most important next step would be to enter a competitive procurement process for a farm partner with whom the early assumptions could be reviewed and refined. The fundraising phase would, ideally, follow the identification of a partner, and the construction phase would be implemented in close collaboration with the farm operator.
The question of prototyping was discussed during the development of the project. While piloting the project on a smaller scale, a common suggestion was to start with the development of the least expensive infrastructure of the farm. It was felt, however, that the greenhouse and patient facility, which make up the largest portion of the capital expenses, are key to demonstrate the project’s success. Indeed, it’s anticipated that the impact on patient experience and patients’ mental state will greatly depend on their interaction with the architecture. Nevertheless, a prototyping mentality should be integrated into all aspects of the farm and programme operation during the first few years, in order to assess assumptions against progress accordingly.
This innovative social enterprise model provides a viable and cost-effective opportunity for hospitals to improve patient programming and research while supporting local agriculture and re-establishing a direct connection with local, fresh food.
Authors
Adeline Cohen is a senior fellow at OpenLab, University Health Network (UHN). Ryan Turnbull is founder and president of Eco-Ethonomics. Kendra Delicaet is an independent research consultant. Edward Rubinstein is director – environmental compliance, energy, and sustainability at UHN. Megan Torza is a partner at DTAH architects. Co-authors also include Phil Mount, Kathleen Camaya and Brenda Nistor.
References
- Raine, KD, Atkey, K, Olstad, DL, Ferdinands, AR, Beaulieu, D, Buhler, S, Campbell, N, Cook, B, L’Abbé, MR, Lederer, A, Mowat, D, Maharaj, J, Nykiforuk, C, Shelley, J, and Street, J. (2018). Healthy food procurement and nutrition standards in public facilities: evidence synthesis and consensus policy recommendations. Health Promotion and Chronic Disease Prevention in Canada. doi.org/10.24095/hpcdp.38.1.03
- Government of Canada (2016). Canada Gazette 2 Nutrition Labelling. Retrieved Fall 2017 from http://gazette.gc.ca/rp-pr/p2/2016/2016-12-14/html/sor-dors305-eng.php
- Vanderlee, L, Goorang, S, Karbasy, K, Schermel, A, and L’Abbe M. (2017). Creating healthier food environments in Canada: Current policies and priority actions – Ontario report. Toronto; University of Toronto, 2017. Available at: www.labbelab.utoronto.ca/Food-EPI-Canada-2017
- Raine, KD, Atkey, K, Olstad, DL, Ferdinands, AR, Beaulieu, D, Buhler, S, Campbell, N, Cook, B, L’Abbé, MR, Lederer, A, Mowat, D, Maharaj, J, Nykiforuk, C, Shelley, J, and Street, J. (2018). Healthy food procurement and nutrition standards in public facilities: evidence synthesis and consensus policy recommendations. Health Promotion and Chronic Disease Prevention in Canada. doi.org/10.24095/hpcdp.38.1.03
- Jones, A, Veerman, J, and Hammond, D. (2017). The health and economic impact of a tax on sugary drink in Canada (summary). Waterloo (ON): University of Waterloo. Available from: www.diabetes.ca/getattachment/Newsroom/Latest-News/Will-a-sugary-drinks-levy-benefit-Canadians/The-Health-and-Economic-Impact-of-a-Sugary-Drinks-Tax.pdf.aspx
- Michaud, P, Condrasky, M, and Griffin, S. (2007). Review and application of current literature related to culinary programs for nutrition educators. Topics in Clinical Nutrition. 22(4); 336–348.
- Scharf, K, Levkoe, C, and Saul, N. (2010). In every community a place for food: the role of community food center in building a local, sustainable and just food system. Metcalf Food Solutions. 2010.
- Elson, PR, Hall, P, and Wamucii, P. (2016). Canadian National Social Enterprise Sector Survey Report. Enterprise Non-Profit Canada. Retrieved from: https://ccednet-rcdec.ca/sites/ccednet-rcdec.ca/files/final-national-report-may-16-2016.pdf
- Toronto Rehab’s Strategic Plan 2016-2021. Retrieved from: www.uhn.ca/TorontoRehab/About/Documents/TorontoRehab_2016_2021_strategic_plan.pdf
- Bill 36: Local Food Act. (2013). First reading 25 Mar, 2013, 40th legislature, 2nd session. Retrieved from the Legislative Assembly of Ontario website: www.ontla.on.ca/web/bills/bills_detail.do?locale=en&BillID=2754&detailPage=bills_detail_status
- Rogerson, M, Brown, DK, Sandercock, G, Wooller, J-J, and Barton, J. (2015). A comparison of four typical green exercise environments and prediction of psychological health outcomes. Perspectives in Public Health. doi:10.1177/1757913915589845
- Kuo, M. (2015). How might contact with nature promote human health? Promising mechanisms and a possible central pathway. Front Psychol. 2015; 6: 1093. Published online 25 Aug 2015. doi: 10.3389/fpsyg.2015.01093
- Hale, J, Knapp, C, Bardwell, L, Buchenau, M, Marshall, J, Sancar, F, and Litt, JS. (2011). Connecting food environments and health through the relational nature of aesthetics: Gaining insight through the community gardening experience. Social Science & Medicine. 72; 1853–1863.
- Wakefield, S, Yeudall, F, Taron, C, Reynolds, J, and Skinner, A. (2007). Growing urban health: community gardening in southeast Toronto. Health Promotion International. 22; 92–101.
- Davies, G, Devereaux, M, Lennartsson, M, Schmutz, U, and Williams, S. (2014). The benefits of gardening and food growing for health and wellbeing. London, England: Garden Organic and Sustain.
- Stavros, E, and Yukht, J. (2014). The health benefits of nature: green spaces play a vital role in patient health. Integrated Health Practitioners. 2014; 55–58.
- Mount, P, Varangu, L, Wylie-Toal, B, Knezevic, I, Cohen, A, Quenneville, L, and Rendek, K. (2017). Ontario public institutions and on-site food production: visualizing the future for healthcare. Guelph, Ontario: Ontario Ministry of Agriculture, Food and Rural Affairs. Available at: http://projectsoil.ca/project-reports/
- Osterwalder A, and Pigneur, Yves. (2013). Business Model Generation. Hoboken, NJ: Wiley.
- Heifetz RA, Grashow A, and Linsky M. (2009). The Practice of Adaptive Leadership: Tools and Tactics for Changing Your Organization and the World. Harvard Business Publishing.
Organisations involved