
Healthcare / Sustainability
Grey Base Hospital case study: resilient, multi-use design in one of the most challenging locations on Earth
By Kris Noiseux, Adam Flowers, Mark Newsome and Margo Kyle | 18 Jul 2019 | 0
This case study presents the challenges and innovative solutions for providing a new secondary hospital and co-located integrated family health centre (IFHC) – Te Nikau Grey Hospital and Health Centre – for the community of Greymouth and wider West Coast region in New Zealand.
Greymouth is a seaside city located on the west coast of the South Island in New Zealand. The West Coast is subjected to intense storms off the Tasman Sea and sits dangerously close to the Alpine Fault. The existing facility was built in the 1960s and is no longer fit for the purpose of the delivery of contemporary healthcare. Portions of the facility are also seismically compromised and are therefore a risk to staff, patients and the community. The facility serves as the secondary hospital for the entire West Coast region, which has a current population of under 33,000 people and a total area of just over 22,000 square kilometres, similar in size to Wales with nearly 100 times fewer people.
The West Coast region is a challenging location to provide health services owing to geological and meteorological extremes. Every year, on multiple occasions, it’s cut off from the rest of the country and tertiary services because of extreme weather events closing the alpine passes, and flooding closing bridges both north and south of the region that allow coastal access. The seismically active area also necessitated that the post-disaster functionality of the facility was a primary design objective.
The new facility, commissioned by the Ministry of Health in New Zealand on behalf of the West Coast District Health Board (WCDHB), was required to have resilient clinical services, designed to allow the health system to be able to respond to the unpredictable high and low variances in demand across the range of secondary health services, in an innovative financially and clinically sustainable way. In addition, the model of care prescribed the integration of primary care, so the facility needed to provide space for general practice clinics, allied health, other general and specialist services, and even a dental suite. These spaces were all designed to be highly flexible, with boundary areas between departments able to be easily reconfigured for influxes of patients, following the philosophy of ‘long life, loose fit’.
The building life span was specified as 50 years, which created a significant challenge in the architectural shell design, detailing, material selection and construction when considering seismic risk and performance during even small earthquakes. This required innovative design solutions for the architecture movement joints, structural design and services reticulation. Adding to the difficulty was the location of the facility, less than 400m from the ocean. The existing facility building fabric and services all have significant corrosion issues, as salt-laden air is frequently driven deep inland with the prevailing winds, and during winter salt spray easily reaches all exposed surfaces around the entire site.
 The original design brief required the facility be constructed to Importance Level 4 (IL4), a New Zealand designation that means the facility has to be fully operational immediately after a one-in-500 year earthquake. The site is located close to the Alpine Fault, which is expected to rupture within the next 30 years, producing a magnitude 8 earthquake. Designing and constructing a facility that is fully functional after an IL4 event requires a significant amount of additional capital investment. The post-disaster management plan for such an event recognised that the district health board doesn’t have sufficient capability to provide large-scale emergency medical services following a major disaster, as it lacks the ‘business-as-usual’ workforce to provide these services. The complex or planned surgeries and clinical care will be transferred to other larger tertiary centres in accordance with local, regional and national disaster-response frameworks in place.
The original design brief required the facility be constructed to Importance Level 4 (IL4), a New Zealand designation that means the facility has to be fully operational immediately after a one-in-500 year earthquake. The site is located close to the Alpine Fault, which is expected to rupture within the next 30 years, producing a magnitude 8 earthquake. Designing and constructing a facility that is fully functional after an IL4 event requires a significant amount of additional capital investment. The post-disaster management plan for such an event recognised that the district health board doesn’t have sufficient capability to provide large-scale emergency medical services following a major disaster, as it lacks the ‘business-as-usual’ workforce to provide these services. The complex or planned surgeries and clinical care will be transferred to other larger tertiary centres in accordance with local, regional and national disaster-response frameworks in place.
This approach allowed for the main facility design to be reduced to an IL3 level, which allows for the building to be non-functional but still preserve life after a natural disaster. The adjacent single-storey IFHC included in the project was designed to IL4 levels and designated as the triage space in the event of a natural disaster. The IFHC would have control of the reception, triage, stabilisation and documentation of casualties, as well as those requiring inpatient care, and provide treatment and discharge of minor casualties.
Besides the challenges provided by the location, there were significant budgetary considerations that had to be carefully considered, as alluded to above. Health spend per capita is significantly less in New Zealand than in the United Kingdom ($3379 NZD versus $5631 NZD, respectively). Even with the reduction of post-disaster functionality of the main facility, the budget was a significant driver for the project. Comparative whole-of-life costings were carried out on all of the major plant, equipment and systems as part of the decision-making process during design. This was to ensure we were providing a financially sustainable solution that could fit within the project budget and be serviced by the DHB for the life of the assets.
The architectural and health planning design was influenced heavily by both the clinical staff and local key stakeholders gathered during multiple user group sessions during the design process. The facility was designed to support the guiding principles of hospitality, generosity, spiritual connectivity, community, family and unity of purpose. These are important considerations for the local community, which consists of a mixture of both European heritage and local indigenous Māori. The facility design was also seen to be an enabler for the implementation of the WCDHB model of care. The model of care represents an integrated health system that is clinically and financially viable, places the patient at the centre of care, and supports people to stay healthy and well in their own community.
The location selected was a green field area on the existing site, however, the boundaries of an estuary to the west, a railway line to the east, the existing hospital facilities to the south, and flood plain analysis meant that careful consideration was needed for the location and orientation of the new buildings. Separate entrances were established for maternity, emergency department and day surgery. The sloped site meant that the main entrance is actually on the first floor, and a direct one-flight up and one-flight down relationship was established in the main public atrium to provide vertical connection. The public lifts were kept completely separate from the clinical lifts to ensure public flows were kept separate from patient flows wherever possible. This is particularly true in departments requiring 24-hour access, and lock-down capability has been provided in these areas to ensure public access is limited to only where it is needed. 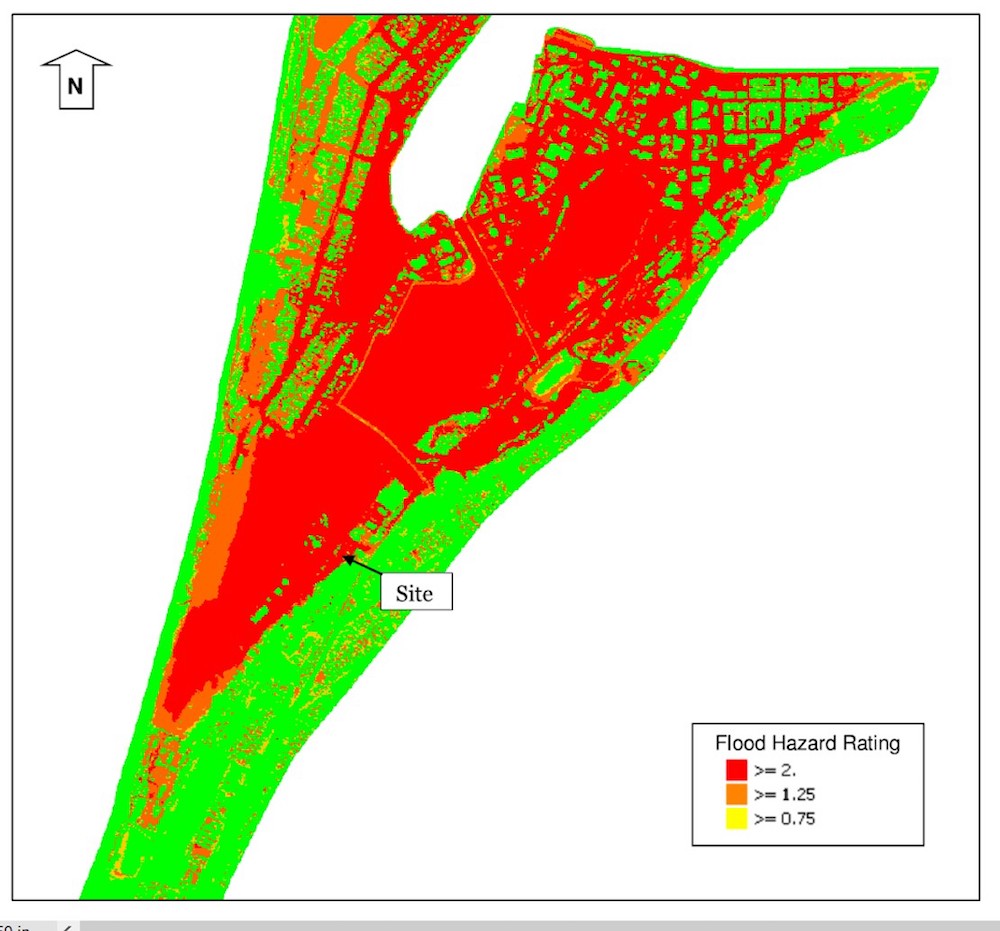
Access to natural light and natural ventilation where possible is a key driver for the design of this facility. An external courtyard between buildings provides greenery for internal facing areas, typically public spaces, while patient spaces have been oriented to provide views of the ocean and the southern alp foothills. All patient rooms are equipped with openable windows for natural ventilation. The West Coast climate is temperate, which allows for the use of natural ventilation in many areas of the hospital. Natural ventilation reduces capital and operational costs but is also more environmentally friendly than providing mechanical ventilation, which requires heating and cooling.
As the facility is remote, rural and supported by the larger, East Coast Canterbury DHB in Christchurch for tertiary and specialist services, the inclusion of staff conference resources for education, teleconferencing and tele-health was another key consideration. This supports the DHB’s operational model and aspiration to support their own talent locally.
 Perhaps the most significant driver in respect to the WCDHB’s ability to successfully implement a modern model of care, build financial sustainability, and maintain the budget for the project is flexibility. This applies not only to the health planning of the facility but also to site services, building services, facade design and traffic planning. Flexibility within the facility means sharing spaces between departments, including inpatient rooms where possible, and ensuring boundary flex spaces are equipped to handle multiple functions. Site flexibility means that interior flows can support the use of multiple points of entry to the building in the case of flooding and road closures during natural disasters. Heating plant has not only been designed to allow for multiple fuel sources but also discrete back-up to the IL4 portion of the facility post-disaster. Even the potable water supply includes back-up for the IL4 facility to support triage after a natural disaster. The principle of flexibility also extends into consideration of change of use and future growth. The generic floor plate allows for future refit as health trends change, while the ambulance bay’s concrete pad has been designed to support an MRI, allowing it to be converted to a future MRI suite. The planning response ensured that the ambulance bay was located to the side of the imaging department.
Perhaps the most significant driver in respect to the WCDHB’s ability to successfully implement a modern model of care, build financial sustainability, and maintain the budget for the project is flexibility. This applies not only to the health planning of the facility but also to site services, building services, facade design and traffic planning. Flexibility within the facility means sharing spaces between departments, including inpatient rooms where possible, and ensuring boundary flex spaces are equipped to handle multiple functions. Site flexibility means that interior flows can support the use of multiple points of entry to the building in the case of flooding and road closures during natural disasters. Heating plant has not only been designed to allow for multiple fuel sources but also discrete back-up to the IL4 portion of the facility post-disaster. Even the potable water supply includes back-up for the IL4 facility to support triage after a natural disaster. The principle of flexibility also extends into consideration of change of use and future growth. The generic floor plate allows for future refit as health trends change, while the ambulance bay’s concrete pad has been designed to support an MRI, allowing it to be converted to a future MRI suite. The planning response ensured that the ambulance bay was located to the side of the imaging department.
The inclusion of an IFHC as a separate but connected building is a specific feature of this project as this type of facility is normally used in a community-based healthcare approach. The decision to include an IFHC was taken, in large part, to support the design principles of flexibility and sustainable services. The scope and diversity of the IFHC service in this project demands a multifaceted approach to planning with, at times, conflicting or competing functional requirements within spaces and zones. The functional briefing phase identified two distinct zones, related to health service delivery – planned and unplanned. The planned zone is accommodated in the IFHC, whereas the unplanned zone is within the main building to support its functional relationship with the emergency department. Beyond its day-to-day activity, the IFHC building has been designated as the emergency operations centre and triage centre, as part of the WCDHB Emergency Management Plan. As such, the building and supporting essential services have been designed to meet IL4 seismic accelerations while remaining fully functional. 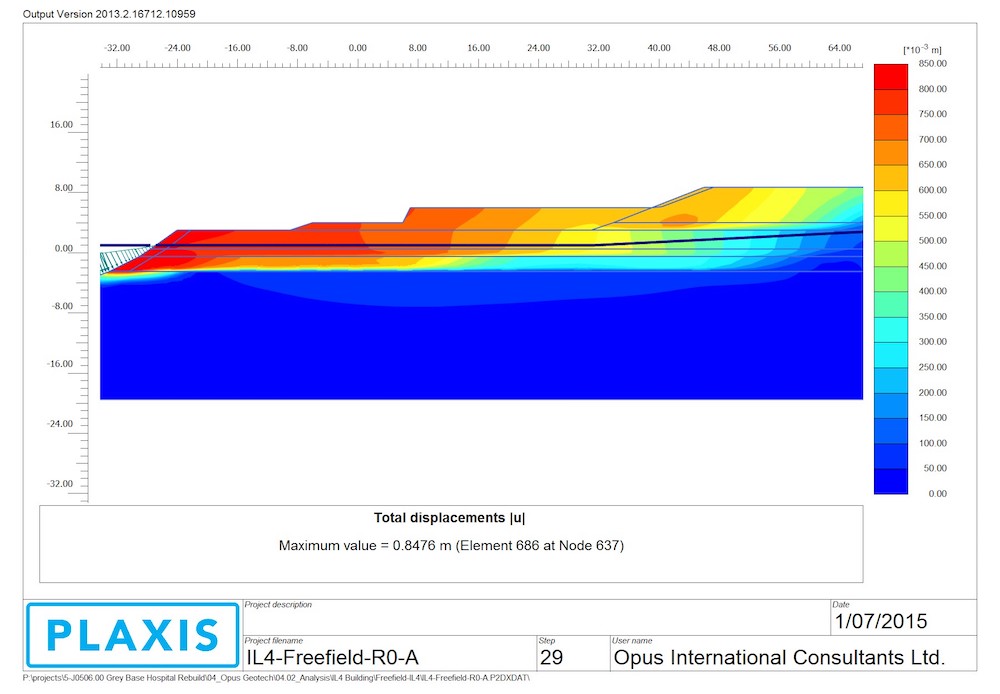
Geotechnical modelling showed that the chosen site was vulnerable to subsidence in a seismic event. There was potential for displacement of more than a metre towards the estuary to the west of the site. In order to ensure compliance with Importance Level requirements, both ground improvement and deep piles were required as part of the ground works. After these remediation measures were taken, the architectural and structural design still had to contend with significant seismic accelerations. The resulting structural design included a seismic gap between the north and south wings of the main facility and seismic gaps between the main facility and IFHC, which are linked by the main entrance on the south side and a corridor to the north. Multiple structural systems were evaluated and consideration was given to procurement times, cost and, most importantly, ease of construction in a remote area such as the West Coast. A steel system, using large concrete ground beams and sliding shoes for the seismic gaps, was selected. The resulting displacements that the shell, facade and building services had to contend with were 75mm between storeys. This proved a challenge but thoughtful consideration to the facade build-up, including a racking tile system, ensured weather tightness could be maintained. Services reticulation used seismically rated flexible connections for all main connections to the buildings and across seismic gaps, while restraint of risers and allowance for inter-storey movement were all included.
Coal mining is a significant part of the West Coast’s history and economy. The existing hospital is one of the coast’s major consumers of coal for the central boiler plant, which produces low-pressure steam for reticulation around the site. The hospital project required a new central energy plant, as the existing boilers are near end of life and the boiler house and stack are seismically vulnerable.
Heating system studies were carried out that considered capital, maintenance and future replacements costs, as well as carbon charges and fuel costs, escalated over 20 years. The cost analysis was overlaid with a study of surety of supply. This was a significant consideration as the alpine passes used for fuel transport are routinely closed due to weather events in winter. Fuel supply then becomes an even greater consideration when one considers that a natural disaster, such as the rupture of the Alpine Fault, would likely close the bridges to the north and south of the city, completely isolating the hospital.
Wood pellet, bio-fuel, diesel, ground-source heat pumps, LPG and coal were all evaluated in detail. The analysis showed that coal was the least expensive fuel, even considering carbon costs, and was the most abundant, accessible fuel available within the city itself. Coal is not a sustainable fuel and is the most carbon dense fuel that could be used. To mitigate this as much as possible, a number of steps were taken. The new coal boiler is sized for peak loading during winter only. The site base, summer and swing season loads are covered by a modulating diesel boiler. This means that the coal system will be completely shut down for four months a year. A cyclonic filter was included to reduce particulate emissions from the coal boiler, and the boiler selection itself uses a screw stoker to allow for simple conversion to wood pellet in the future. There is currently no supply of wood pellets into the South Island, however, this may change in the future. Site storage space limitations meant that wood waste or other bio-fuel was not a viable option. More than 80 per cent of New Zealand’s electrical grid supply is produced by wind or hydro-electric generation, which made ground-source heat pumps an attractive and highly sustainable solution. The technology, however, was deemed to be too high a risk of failure in this highly seismic zone.
The overall load on the central heating plant was reduced as much as by minimising process and building loads. The building incorporates high-performance double glazing, a warm shell-insulated roof, and both internal wall insulation and external foam with a radiant barrier. Overall insulation and glazing thermal resistance values exceed building code minimums by 50 per cent. In order to reduce process heating loads, the sterilisations suite is fully electric, allowing for the central heating plant to be designed to provide low temperature water instead of steam. While steam is an efficient way to transfer heat over long distances, standby losses can be significant.
The temperate climate on the West Coast means that the building cooling demand is not high on a square-metre basis, but must be highly reliable for the main hospital. An internal chiller plant room was created that allowed for high air turnover for the air-cooled chillers. The latest oil-free centrifugal chillers were selected for both low maintenance costs, reliability and noise considerations. Use of natural ventilation in non-clinical spaces in conjunction with the building design successfully reduced cooling loads. A variable primary pumping design and sophisticated control system reduces energy consumption through the entire chilled water circuit even further.

Splitting the resiliency requirements across the main hospital (IL3) and the IFHC (IL4) proved challenging to implement. During normal operations, the IFHC uses the same services infrastructure (water, sewer, medical gases, chilled water, heating hot water, electricity and communications) as the main facility. These services are also shared by a number of buildings around site that are being retained. Designing the services’ reticulation to be fully functional after a one-in-500-year earthquake had a significant increased cost associated.
As an alternative innovative solution, the IFHC was designed to be operational in ‘island mode’ after a significant event and fully functional for 72 hours. To achieve this, an electric boiler was included in the IFHC plant room, providing heating for hot water, as well as potable hot water via a calorifier. Potable water is provided by an IL4-rated water tank installation for the IFHC, and also provides sufficient fire water storage for the building. Power is provided by a diesel generator set, with cable reticulation that allows for ground movement corresponding to an IL4 event. The sewer pump station installed for normal use on the site has sufficient capacity to hold 72 hours of waste water from the IFHC. Communications back-up and emergency response communications are handled by a UHF radio installation. Medical gases, which are essential in a post-disaster scenario, are housed in an IL4-rated bunker with resilient reticulation to the IFHC.
The Te Nikau Grey Hospital and Health Centre exemplifies resiliency in architectural and engineering design planning, required to address a range of geological and meteorological challenges, while working within the constraints of a limited budget in a remote, rural environment. Additionally, the brief was met with the design of the facility viewed as an enabler to successful implementation of the WCDHB integrated model of care, inextricably linking the clinical and financial sustainability of a health service addressing the challenges of delivering a full range of secondary services to a low population across a large, isolated geographical area.
Authors
Kris Noiseux is a technical principal, building services at WSP in New Zealand. Adam Flowers is director at CCM Architects. Mark Newsome is facilities development director and Margo Kyle is facilities integration manager at West Coast District Health Board.
Organisations involved
