Healthcare / Evaluation and performance
ProCure 22 Efficiency and Productivity Programme: pre- and post-occupancy evaluations toolkit
By Rosemary Jenssen, Alan Kondys and Stephanie Williamson | 30 Aug 2018 | 0
This paper describes the ProCure 22 (P22) Efficiency and Productivity Programme’s (EPP) pre- and post-occupancy evaluations toolkit, which can be used to assess realised benefits from UK healthcare projects.
Authors of scientific paper:



Abstract
The ProCure 22 (P22) Ef ciency and Productivity Programme’s (EPP) pre- and post-occupancy evaluation toolkit can be used to assess realised benefits from UK healthcare projects.
Collaboration has been at the heart of the development of this tool, with all six Principal Supply Chain Partners (PSCPs) engaging with the Department of Health, NHS England, NHS Improvement, Principal Supply Chain Members (PSCMs), and NHS trusts, to develop a standardised approach to post-occupancy evaluation (POE), while responding to Lord Carter’s efficiency and productivity drivers. All six PSCPs have committed to ensuring post-occupancy evaluations are undertaken and shared across all of their P22 schemes, at no additional cost to the NHS.
The P22 POE toolkit is available to all to use, without charge. P22 recognised the value in capturing benefits, through measurement and before-and-after assessment, to inform future developments. These common outputs, measured across physical measures – eg, floor areas, workload and activity, functionality and effectiveness, environmental and economic – bring together, in one toolkit, common measures enabling accurate scheme-to-scheme comparison and benchmarking. Current implementation at a national level will result in a body of knowledge and outcome measures, which have the potential to influence both national and international procurement, as well as providing direct comparison of healthcare building performance in use. A key component of the toolkit is the patient and staff surveys, which enable those at the front line experiencing new facilities to have a voice in their assessment.
The pre- and post-occupancy evaluations sit under the umbrella of the Government Soft Landings (GSL) P22 processes. They will be undertaken at appointment, and in years one, two and three following occupation. The data and commentary gathered should support the realisation of evidence benefits, as well as begin to inform and support new developments, while also assisting in identifying trends and areas requiring further design input or research. The potential of this toolkit is significant, both inside and outside of the P22 framework. It also offers an opportunity to demonstrate the UK’s position at the forefront of healthcare design toolkits, guidance and innovation.
Keywords
The ProCure 22 (P22) framework
P22 is a £4bn, four-year construction procurement framework administered by the Department of Health and Social Care (DHSC) for the development and delivery of NHS and social care capital schemes in England. It’s consistent with the requirements of government policy, including: the productivity and efficiency agenda; the Government Construction Strategy; the Public Contracts Regulations 2015; National Audit Office guidance on the use of centralised frameworks; and the Cabinet Office Common Minimum Standards for procurement of the built environment in the public sector.
P22 represents the third iteration (previously P21 and P21+) of the DHSC framework, providing design and construction services for use by the NHS and social care organisations for a range of works and services. P22 continues to build on the principles of its predecessors to streamline the procurement process and create an environment in which clients, Principal Supply Chain Partners (PSCPs) and their supply chains develop stronger partnerships that drive increased efficiency and productivity while supporting enhanced clinical outputs for patients, and improved environments for staff and visitors.
Efficiency and Productivity Programme (EPP)
The collaboration work under ProCure22 has been undertaken under the P22 Efficiency and Productivity Programme (EPP). The programme aims to deliver efficiency and productivity while improving patient outcomes across health and social care, through development of a range of tools offering “added value” and “better value” to healthcare clients while meeting Government Construction Strategy targets.
ProCure21+ and, now, ProCure22 have developed a series of evidence-based and experience-grounded tools, including;
- pre- and post-occupancy evaluations;
- a project-end review;
- a design appraisal toolkit;
- a healthcare colour palette;
- a virtual reality hospital;
- an expanding range of standard component suppliers/manufacturers; and
- 24 repeatable room arrangements.
These are all collaborative efforts delivered not only by the DHSC and six PSCPs but also by NHS Improvement, NHS England, NHS trusts, Royal colleges, patient groups, clinicians, academics, estates teams, Principal and Supply Chain Members (PSCMs), and many other interested stakeholders.
Virtual teams
The framework programmes have been led and developed by virtual teams from across the PSCPs and PSCMs, covering five strands: design (which includes the repeatable rooms, VR hospital, Government Soft Landings, and post-occupancy evaluations); components + assemblies; BIM + the digital estate; data management; and training.
Underpinning these virtual teams have been the DHSC, NHS Improvement, NHS England, NHS trusts, the Royal colleges, the Principal Supply Chain Members, and wider supply chain, which have all provided input to the process, toolkits and products.
Toolkit introduction
Launched in October 2017, the P22 POE toolkit can be used by everyone in healthcare, both before and after development, to assess project benefit targets and benefits realised. Collaboration has, once again, been at the heart of the tool’s development, with all six PSCPs (Kier, IHP – Vinci and Sir Robert McAlpine, Interserve, Galliford Try, BAM and Graham) engaging with the DHSC, NHS England, NHS Improvement, Principal Supply Chain Members and NHS trusts, to produce a standardised approach to POE, encompassing NHS business case requirements, NHS Improvement’s Model Hospital metrics, and responding to Lord Carter’s report into efficiency and productivity drivers for hospitals.
One of the seven key principles for the NHS, set out in its constitution, is that it’s “committed to providing best value for taxpayers’ money and the most effective, fair and sustainable use of finite resources”. Additionally, the NHS is committed to meeting efficiency and productivity targets, outlined in the NHS’ 10-point Efficiency Plan.
To achieve this, business cases are structured to enable their assessment and appraisal to be carried out in accordance with the Treasury’s Five Case Model for business case development:
- Strategic case – to demonstrate that proposals are supported by a robust case for change;
- Economic case – to demonstrate the options appraisal of potential benefits compared with costs, and that value for money has been optimised;
- Commercial case – to demonstrate that proposals are commercially viable;
- Financial case – to demonstrate that proposals are financially affordable; and
- Management case – to demonstrate that proposals can be delivered successfully.
Post-occupancy evaluation (POE) is used to inform, support and capture evidence-based design outcomes to meet the requirements of the Five Case Model.
POE aims and aspirations
The PSCPs recognised that while POEs have been part of the healthcare design, delivery and in-use process for many years, there was a need to support a common pre- and post-occupancy evaluation toolkit that provided:
- PSCP facilitation supporting healthcare clients;
- standardised POE methods and metrics aligned with NHS Improvement’s Model Hospital;
- widely accessible findings and conclusions;
- a focus on technical performance and outcomes related to patient-centred care and staff experience;
- staff and patient consultation so that those working and receiving treatment or care in a new facility could provide input; and
- lessons learned to be shared and communicated.
POE overview
In line with national and local strategy drivers, the P22 framework has developed a pre- and post-occupancy evaluations toolkit, compliant with Government Soft Landings (GSL) standards, to capture outcome measures across a range of areas that the built environment can influence and support. The metrics support ‘before’ and ‘after’ comparison of the healthcare development, across both new-build and refurbishment schemes.
All six PSCPs have committed to ensuring POEs are undertaken and shared across all of their P22 schemes, at no additional cost to the NHS. The P22 POE toolkit is available for all to use, without charge.
The P22 framework marks a step change in approach following on from evidence-based and experience-informed tools, including the repeatable rooms, VR hospital, standard components, and healthcare colour palette.
P22 recognises the value in capturing benefits delivered, through measurement of before and after assessments, to inform current and future developments. The P22 POE common outputs – measured across physical measures such as floor areas, workload and activity, functionality and effectiveness, environmental, and economic – bring together in one toolkit a set of familiar measures enabling accurate scheme-to-scheme comparison and benchmarking.
 Current implementation at a national level will result in a body of knowledge and outcome measures, which have the potential to influence both national and international procurement, as well as providing direct comparison of healthcare building performance in-use.
Current implementation at a national level will result in a body of knowledge and outcome measures, which have the potential to influence both national and international procurement, as well as providing direct comparison of healthcare building performance in-use.
The pre-occupancy evaluation will be undertaken at appointment, with the post-occupancy evaluations undertaken at the end of years one, two and three following occupation. Data and commentary gathered will help evidence the benefits realised, as well as start to inform and support new developments. They will also assist in identifying trends and areas requiring further design input, innovation or research. The PSCPs, supported by the DHSC, have committed to undertaking a POE for each scheme procured under the P22 Framework.
The potential of this toolkit is significant, both inside and outside of the P22 framework, demonstrating the UK’s position at the forefront of healthcare design assurance toolkits, guidance and innovation. 
Toolkit requirements
Communicated through the P22 Framework Instruction no. 13, the POE toolkit is supported by both the P22 POE User Guide (published on the P22 club website – www.procure22.nhs.uk) and by six designated PSCP POE champions.
Pilot assessments have been undertaken across mental health, community and acute health schemes, completed under the P21+ framework, and led by the designated healthcare client and PSCP POE champions. Feedback from these pilots have shaped and informed the final version of the toolkit, now available on the P22 club website.
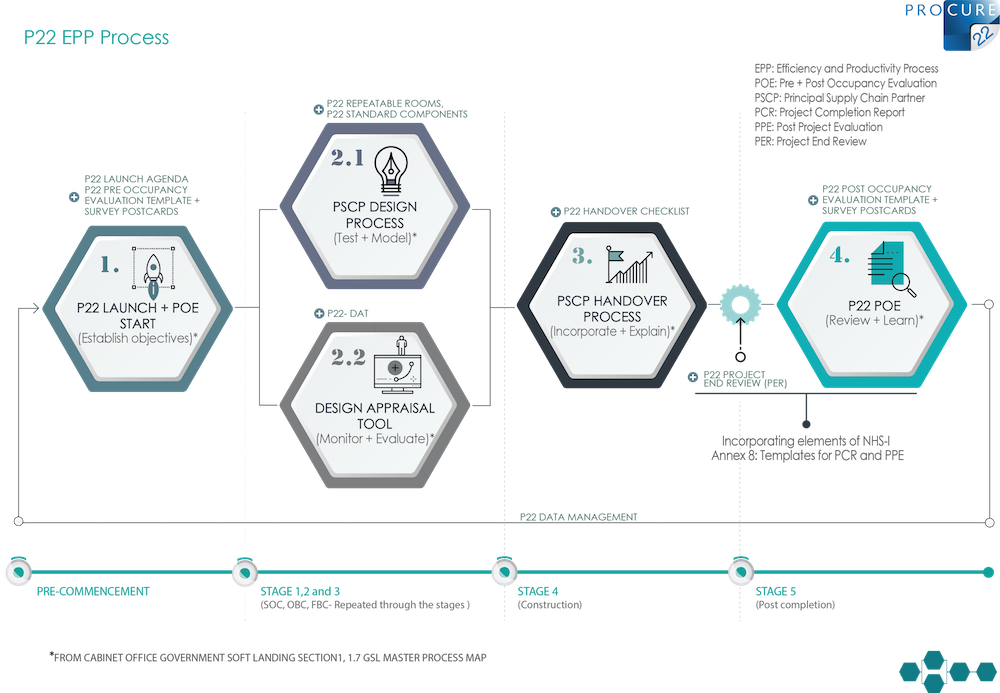
P22 POE process
The P22 POE process starts with a pre-occupancy evaluation to capture the business case benefits and establish the baseline, including NHS efficiency and productivity targets, by which the project will be measured. Ideally undertaken at the initial briefing/design stage, the pre-occupancy evaluation may be completed at any stage prior to the development being occupied. Once the pre-occupancy evaluation has been undertaken, the realised benefits of post-occupancy can be measured, evidenced and compared (see Figure 5, outlining the P22 POE process). 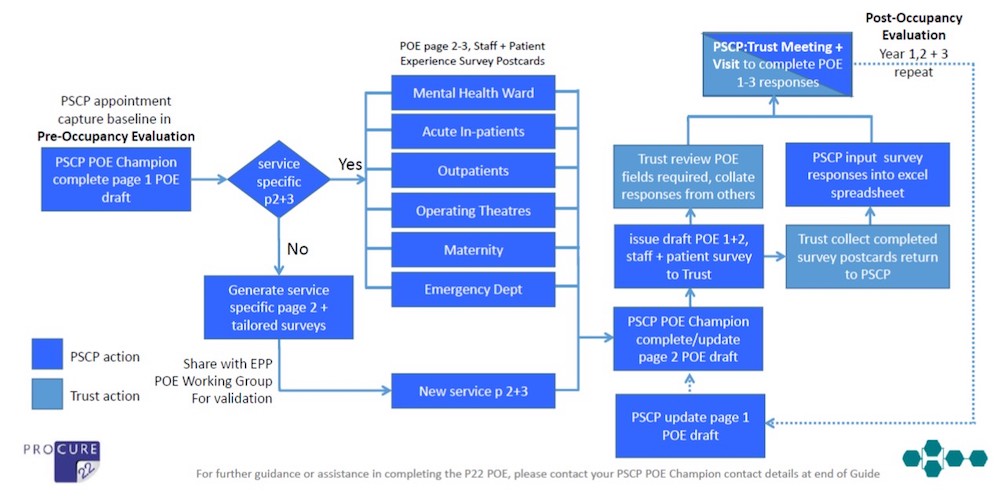
A PSCP POE champion (named in the User Guide) provides support to help NHS clients and their PSCP team complete the assessments at a local level. To successfully complete the POE, input will be required from several disciplines – including patient, carer, staff and building user surveys and metrics – with the project POE champion and NHS client POE lead working together as a single point of contact.
Data and, importantly, the associated commentary will be captured over a three-year post-occupancy period, enabling the building's performance to be assessed at 12 months, 24 months and 36 months.
P22 POE toolkit components
The toolkit comprises a set of standard pro-forma documents that apply across all schemes, a set of service-specific documents, together with corresponding sets of easy-to-complete survey feedback postcards for patients, carers, staff and users. 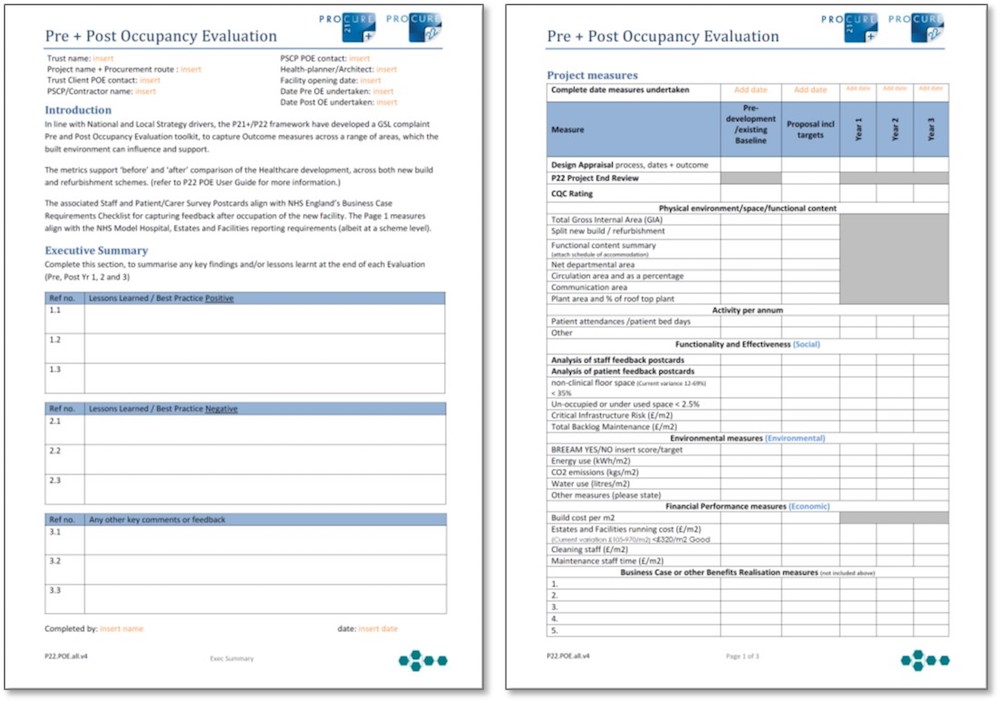
Documents are currently available for:
- acute inpatient wards;
- maternity units;
- mental health inpatient wards;
- outpatients;
- operating theatres;
- urgent care and emergency departments; and
- special care baby units or neonatal intensive care units.
For clinical services not listed above, a service specific pro-forma will be developed by the P22 PSCP with the support of the working group. Once approved, this will be shared to expand the menu of services covered. Service-specific documents currently under development by the EPP Working Group include: endoscopy; renal dialysis units; critical care in-patient units; and imaging and diagnostics. 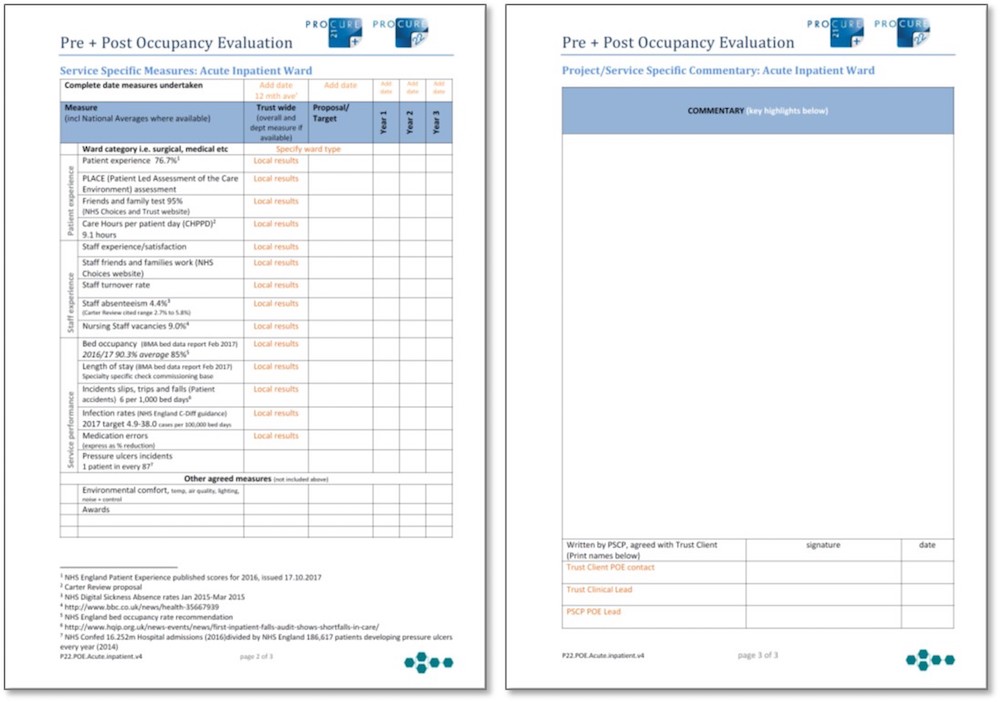
Key components of the POE toolkit are the patient and staff surveys, enabling those at the front line experiencing new facilities to have a voice in the assessment in use. A standardised two-page format captures all survey responses in an ‘at a glance’ report. This can be shared following completion of the surveys for the participants to be appraised of the feedback and appended to the POE pro-forma. While this approach recognises the importance of metrics and measures, statistics need to be supported by clear commentary and explanation. 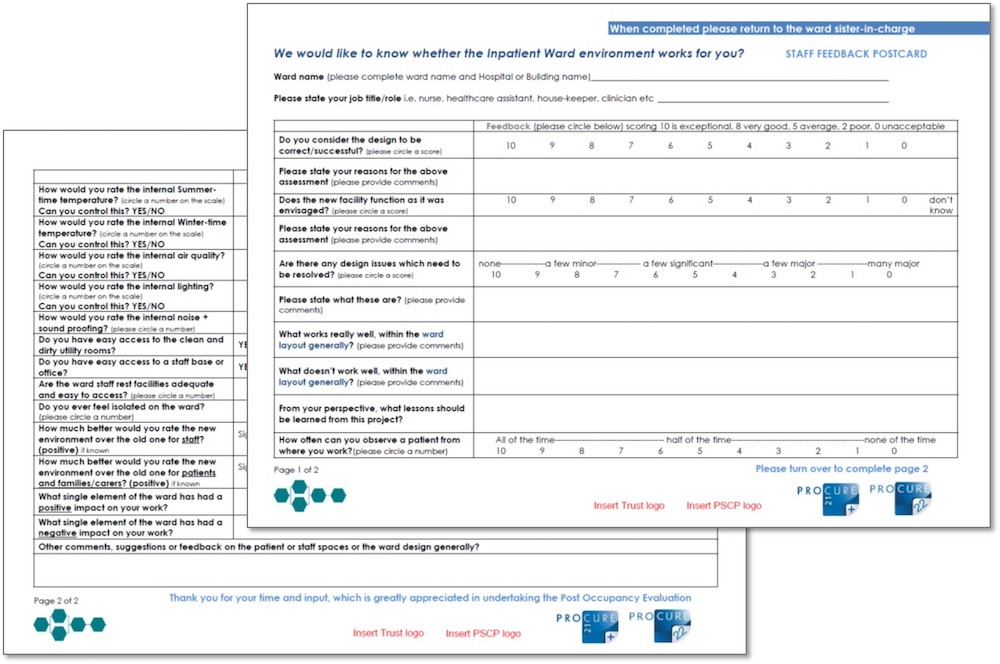
POE toolkit: next steps
Currently the POE pro-forma and survey postcards are available as word format documents. The data working group is developing online versions that will be directly linked to the P22 club website’s Projectshare database, which will be launched later in 2018. This will support:
- easier access and completion of the pro-forma;
- pre-populated project information;
- links to P22 MMS messaging for live status updates on POE completion;
- the facility for automated benchmarking data; and
- automatic uploading of the executive summary page once agreed.
More recent POE pilots have successfully used online survey platforms in place of hard-copy postcard surveys for collecting staff and patient feedback (see Italian Hospital case study).
P22 post-occupancy evaluation case study: Atherleigh Park P21+, North West Boroughs Healthcare NHS FT
Before its official launch, the POE toolkit was trialled by six PSCP POE champions across separate pilot schemes. One such pilot was Atherleigh Park mental health hospital in Leigh. Here, a new build had set out to deliver a new model of care with high-quality services in a suitable environment that met the expectations of the service user and carer, and delivered local services through a skilled and motivated workforce.
 The pilot POE was undertaken six months after occupation of the new facility, supported by Rosemary Jenssen as the PSCP POE champion, and Paul Jackson as the healthcare client POE lead. It required considerable effort, from the trust staff, the PSCP and the architect to track back through the life of the project, commencing with a strategic outline case (SOC) in 2012, with the facility completed and occupied in March 2017. Had the pre-occupancy evaluation pro-forma been available in 2012, the task of establishing the baseline to measure the development performance against would have been much easier.
The pilot POE was undertaken six months after occupation of the new facility, supported by Rosemary Jenssen as the PSCP POE champion, and Paul Jackson as the healthcare client POE lead. It required considerable effort, from the trust staff, the PSCP and the architect to track back through the life of the project, commencing with a strategic outline case (SOC) in 2012, with the facility completed and occupied in March 2017. Had the pre-occupancy evaluation pro-forma been available in 2012, the task of establishing the baseline to measure the development performance against would have been much easier.
The POE gathers information around lessons learned, positive and negative, as well as specific data, other comments, feedback and areas where more work may be needed. It embeds the voice of the patient and front-line staff both pre- and post-completion of the project. 
The POE itself took the form of desktop pre-population of the key performance data, data received from the trust, and a one-day on-site evaluation with the healthcare client POE lead, the trust clinical lead, the PSCP POE champion, and the architect in attendance. This comprised: a series of departmental walkarounds and visits; one-to-one interviews, including with clinical service leads, estates, security, infection prevention, fire, facilities and managers; participation by 19 service users across the two adult acute wards; and completed surveys by more than 60 ward-based staff members. Through use of the P22 POE toolkit and pro-forma, more than 100 individuals (staff and service users) shared input as part of the POE.
The pilot schemes proved that POEs shouldn’t be undertaken in isolation. The POE process and toolkit, however, provide a consistency of approach to undertake pre- and post-occupancy evaluations across all schemes. 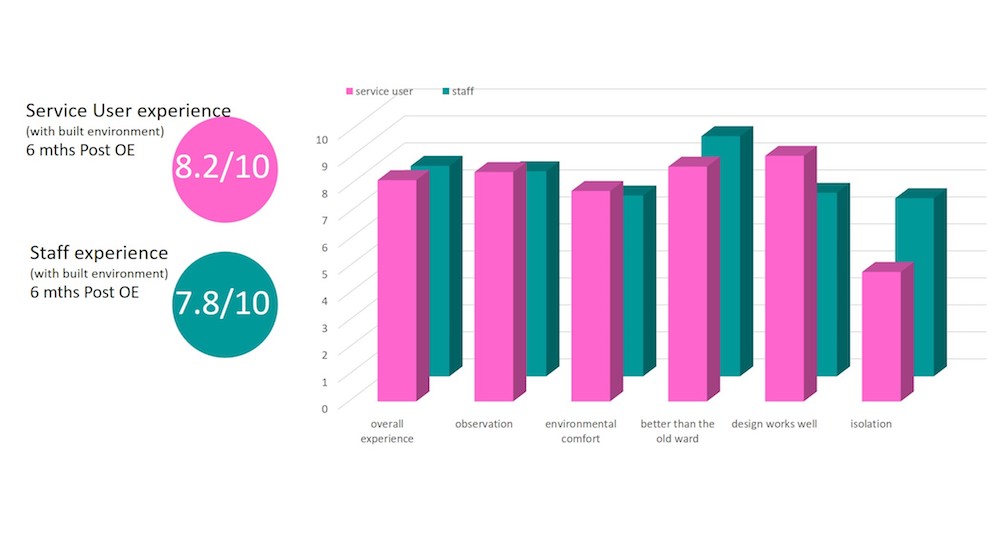
The toolkit highlighted a number of positive results, including:
- 23 per cent more patients are being treated each year with only 8 per cent more beds (compared against 2012 figures as baseline);
- bed occupancy has reduced from 90 per cent to below the Royal College of Psychiatrists’ recommendation of 85 per cent;
- the building’s energy use has decreased significantly, to less than a third of its 1980s predecessor – despite the new facility being marginally larger – with a corresponding decrease in CO2 emissions and water use; and
- survey responses from service users and staff reflect an average 8/10 score (very good) for experience and satisfaction with the environment.
P22 post-occupancy evaluation case study – St Ann’s Hospital P21+, Poole
IHP also trialled the POE toolkit with Dorset Healthcare NHS Foundation Trust on the completed St Ann’s Hospital mental health facility in Poole.
This facility is a new-build, two-storey unit consisting of a 16-bed and 14-bed ward, with assessment, treatment and support rooms. Featuring a new entrance, contemporary landscaping and the redevelopment of existing car parks, the new building is located on the site of outdated facilities built in the 1970s and 1980s and now demolished. 
This POE was undertaken by Alan Kondys, supported by Rosemary Jenssen along with Kerri Howlett from the trust, with as much advance pre-population of the template as possible.
Service-user and staff postcards were distributed in advance of a half-day workshop, when the data were scrutinised and the findings summarised.
An interesting aspect of this trial, three years after occupation, is that it followed on from an informal, bespoke POE undertaken after year two. This enabled identification of the toolkit’s following key benefits:
- Whereas the year-two POE considered and identified clear improvements in service provision and building efficiency, these improvements were not able to be benchmarked against how the old building performed or against stated objectives for the new facility. The P22 POE toolkit, however, provides for establishing these benchmarks aligned with the project objectives.
- Although the year-two POE did consider the positive service user and staff feedback, this was based on what was known by the limited number of attendees at the POE meeting. The year-three POE, using the P22 toolkit, involved distributing the service user and staff postcards, which provided broad and direct feedback. Indeed, a memorable aspect of the POE was the eagerness of staff to attend the review to hand over their completed postcards.
Equally notable were the results from the completed service-user and staff postcards (see Figure 12). 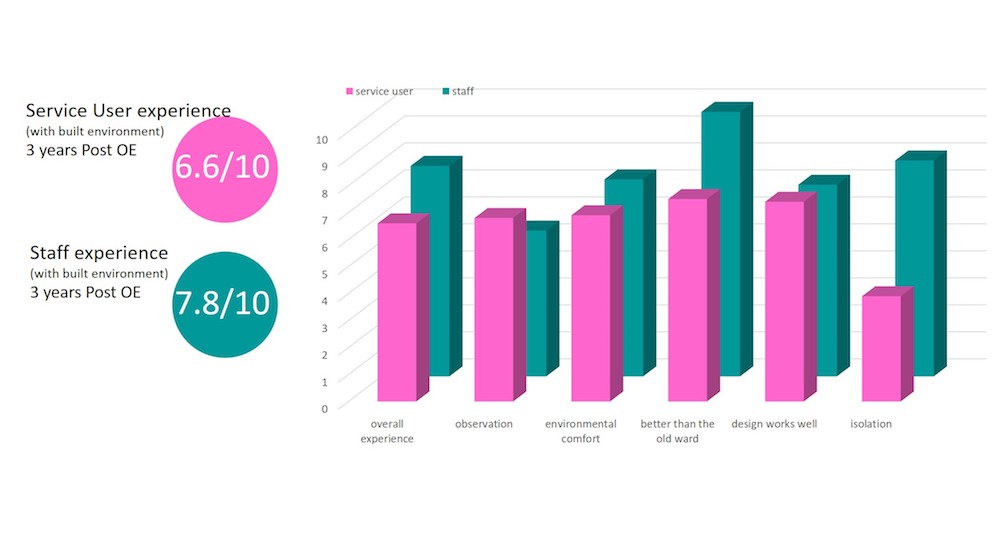
For service users:
The highest scoring feedback was recorded for the question “Do you consider the design of your bedroom works well?”, which scored 80 per cent. This supported the objective to create rooms to meet service-user requirements. The lowest score was recorded for the question “Do you ever feel isolated or lonely in the ward?”, which scored 38 per cent. This was thought to reflect service users spending more time in their new bedrooms and has enabled staff to respond positively to this.
For staff:
The highest scoring feedback was for the question “How much better would you rate the new ward over the old one for patients?”, which scored 98 per cent. The reasons cited – service users being less distressed by the new environment, and an integrated high-level courtyard providing unsupervised access – offer lessons for good practice.
The lowest score was for the question “Do you have easy access to a staff rest room?”, which scored 58 per cent. Although this wasn’t a particularly low score, it has encouraged consideration of how this area can be improved in the way the building is used.
It’s thought that use of the P22 POE toolkit at the start of the design process will assist the team in meeting the scheme aspirations. The tool enables the recording of pre-development and pre-occupancy benchmarks, as well as clear objectives, which focuses the whole team on what needs to be achieved and what the outcome will be measured against at 12, 24 and 36 months after occupation.
P22 pre-occupancy evaluation (pre-OE) case study – the Italian Hospital redevelopment into a new Sight and Sound Centre for Children, Great Ormond Street Hospital for Children NHS FT (GOSH)
The pre- and post-occupancy evaluation toolkit is now in use across all P22 schemes. Among the first schemes to be awarded under the P22 framework was a programme of works for Great Ormond Street Hospital for Children in London. This included the Italian Hospital, a re-development of a Grade two listed building at Queen Square in central London, designed by Sonnemann Toon Architects. The project itself commences on site this summer with an anticipated completion early in 2020. 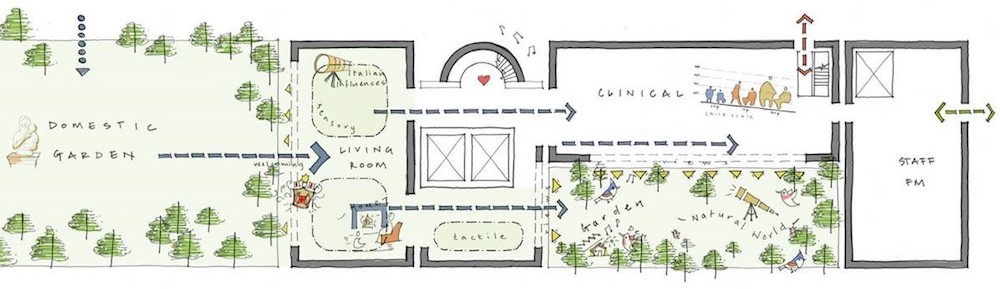
GOSH’s nominated POE champion, Emma Hau, (a healthcare planner in GOSH’s property and development directorate) worked alongside her colleagues at GOSH, and was supported by Kier POE champion Rosemary Jenssen, to complete the pre-occupancy evaluation of the scheme.
Through GOSH’s communication team, the patient and parent survey postcard questions were tailored to ensure a child-focused approach. The postcard survey format for both staff and patients/carers was developed into an online version using Survey Monkey. Invitations to participate in the survey were sent out to all the centre’s current patients, parents/carers and staff. Using this format elicited 231 responses over a four-week period. 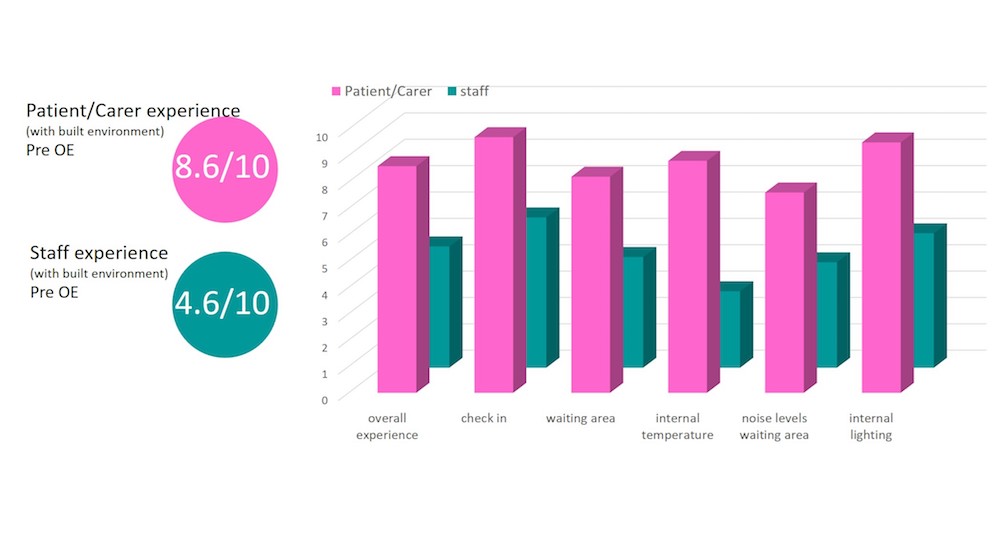
Prior to the P22 appointment the trust had already undertaken significant engagement and consultation across a wide range of stakeholders, including patient groups and the Young People’s Forum. The POE toolkit enabled the team to reflect on the current environment to reflect on how it needs to support, at a detailed level, the needs of those working and receiving treatment in the new Sight and Sound Centre. During the pre-occupancy evaluation stage, a number of environmental factors had been raised as particularly important for this patient group, including acoustics, noise, and the natural and artificial lighting strategy and levels. The toolkit provided a platform to record “other agreed measures”, which involved measuring the noise and lighting levels in the existing waiting areas.
The level of goodwill and generosity demonstrated by individuals in taking the time to complete the survey led to the development of an ‘at a glance’ report-back format, so that the findings could be shared with those who had participated in the process. In this way, concerns over survey fatigue and a feeling that responses might “get lost in the ether” were overcome. The completed pre-occupancy evaluation is serving as a useful tool against which design development decisions can be measured, as well as to keep the team focused on the main purpose of the facility and the trust’s benefits to be realised for patients, families, carers, staff and wider stakeholders. 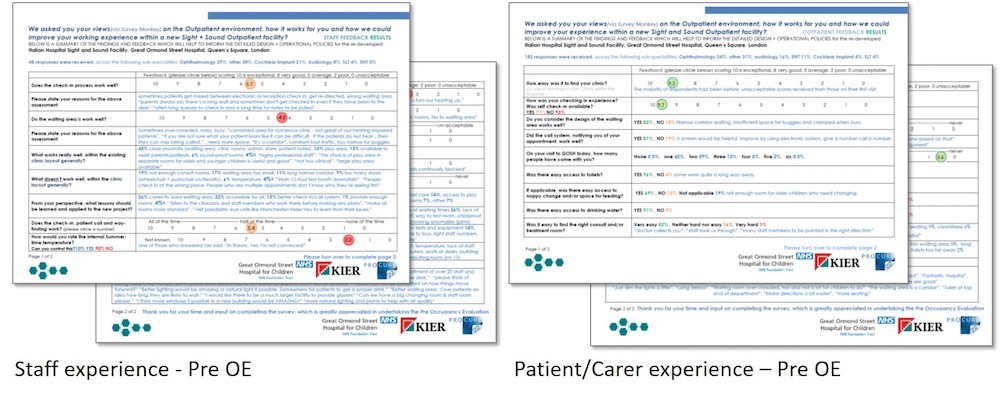
This new innovation in the toolkit, developed for GOSH, is now being rolled out across all other P22 POEs. It goes beyond the baseline score of the existing facilities of 4.6 out of 10 by staff and 8.6 out of 10 by patients/parents/carers, and provides great insight into the experiences of those using the facilities. Unsurprisingly, a parent/carer’s focus is on receiving expert treatment and care, and they appear less critical of the existing environment than those spending their working days in the same space. The detail and the comments provided are nevertheless helpful in shaping the new facility.
For GOSH, it’s increasingly important to collect this data early in order to validate the benefits realisation of its capital schemes, develop its own expertise at design briefing and delivery, and support its commitment to enhance the patient environment and experience.
Authors
Rosemary Jenssen BSc (Hons), BArch (Dist), ARB, RIBA is director of Jenssen Architecture. Alan Kondys FRICS is framework director for Integrated Health Projects, and health sector director at Vinci Construction UK. Stephanie Williamson BSc MA is deputy director of development at Great Ormond Street Hospital for Children.
Acknowledgements
The paper has been produced for and on behalf of the P22 Principal Supply Chain Partners (PSCPs).
References
No references