Healthcare / Service redesign
Western HealthLinks
By Craig Nelson, Robert Rothnie, Jason Plant, Dr Arlene Wake and Russell Harrison, CEO | 13 Sep 2018 | 0
This paper provides an evaluation of Western HealthLinks – a chronic illness management programme providing support for high-risk patients with chronic and complex conditions in the community.
Authors of scientific paper:
Abstract
Western Health Healthlinks is a chronic illness management programme providing support for high-risk patients with chronic and complex conditions in the community. Launched in November 2016, Healthlinks is funded by the Department of Health and Human Services (DHHS) in Victoria, Australia. It explores how flexible funding for the chronic illness group can facilitate changes in service delivery. The Healthlinks model of care has been formulated through an extensive literature review, benchmarking and consultation process.
Application: The package of chronic illness interventions at Western Health includes: identification systems; advanced discharge programme; post-discharge support programme; 24/7 registered nurse phone support; ‘hospital-like’ clinical care in the home; care co-ordination and navigation; primary care integration; post-discharge pharmacy review; e-health; advanced care planning; and integrated collaborative strategies.
Aim: The primary aim of the evaluation of this programme is to determine if the model of care affects the number of days alive not admitted to hospital. Secondary aims include examining the impact of the model of care on healthcare costs, service use and patient experience.
Methods: The evaluation of the Healthlinks programme will examine the effects of a cohort receiving the chronic illness management programme compared with a cohort receiving standard care. Data will be analysed for the intervention group and compared with the control health service, including:
- Data set A: days alive, not admitted to hospital (episode data);
- Data set B: economic cost (cost of services provided) and service use (episode data); and
- Data set C: patient experience (survey and quality of life).
A 12-month detailed analysis of an innovative community chronic care programme will be presented compared with a control health service. Early analysis suggests decreased acute healthcare utilisation compared with that predicted, but the control comparison will inform the true evaluation of the programme and its potential benefit for healthcare and society.
Results: A detailed analysis of 12 months of the programme will be presented. Preliminary analysis suggests a 27-per-cent reduction in acute healthcare utilisation at 11 months.
Implications: We intend to present a formal evaluation of the programme.
Keywords
This paper provides an evaluation of Western HealthLinks – a chronic illness management programme providing support for high-risk patients with chronic and complex conditions in the community.
Western HealthLinks is a pilot programme supported by the Victorian Department of Health and Human Services (DHHS). The pilot operates on the assumption that integrated, co-ordinated care can result in better health outcomes for people living with chronic disease. There is also recognition that current funding mechanisms can prevent health services from providing a cohesive and co-ordinated model of care that integrates hospital, ambulatory and community-based services. Western HealthLinks aims to remove some of those barriers, enabling the trial of an innovative model of integrated care.
Western Health
Western Health (WH) provides comprehensive health services for the community of western Melbourne. WH employs more than 6000 staff and provides a wide range of services from acute tertiary services in the areas of emergency medicine, intensive care, medical and surgical services, through to sub-acute care, specialist ambulatory clinics, drug and alcohol services, and community-based services. WH is also a key provider of maternity, paediatric and cardiac services.
Our catchment
In the western region of Melbourne in Victoria, Western Health (WH) serves one of the fastest growing populations in Australia. From a current population of approximately 1 million people, the western growth corridor is expected to grow by around two-thirds over the next 10 years to in excess of 1.42 million people, an increase of more than 400,000. WH also sees a higher proportion of older residents than the national average, with more than 90 per cent of all non same-day patients aged over 70. 
Similar to the size of greater London at more than 1560 square kilometres, the region is one of the most culturally and linguistically diverse communities in Australia. More than 110 languages are spoken, and nearly 50 per cent of the population speak a language other than English at home. People from over 130 different nations now call the western region of Melbourne their home.
With a 39-per-cent higher unemployment rate than the national average, lower than average labour workforce participation, and a large proportion of residents living below the poverty line, our community faces significant socio-economic challenges. With a high reliance on the public health system, the region also has low numbers of general practitioners (GPs) per head and low rates of private health insurance.
Our community also experience poor outcomes across a range of health indicators. Specifically, our catchment has higher rates of: overweight and obesity; type 2 diabetes; high blood pressure; smoking; physical inactivity; and children who are developmentally vulnerable on one or more domains. WH is aware that patients with chronic illness are associated with a greater risk of poorer health outcomes and premature death, use health services more frequently, and account for a greater percentage of healthcare costs.1 The main conditions leading to health burden are: coronary heart disease; pain; chronic obstructive pulmonary disease; and lung cancer – which, combined, contribute to 18 per cent of the total burden, with at least 31 per cent of this burden considered preventable.2 At WH, the 30-day readmission rate for chronic illness, such as chronic heart failure, chronic obstructive pulmonary disease, diabetes and renal failure, is between 19 and 24 per cent, which is comparable to international benchmarks,3 but doesn’t provide a satisfactory outcome for patients.
The DHHS HealthLinks pilot
Australia uses an activity-based funding model to support the provision of public hospital services. Activity-based funding (ABF) pays hospitals based on the number and mix of patients they treat. If a hospital treats more patients, it receives more funding.4
While ABF is an effective funding model for short-term episodic care, it’s less effective for supporting the delivery of long-term, proactive and systemic care approaches.4 With patients challenged with chronic and complex illness identified as being at risk of poorer outcomes and being a greater healthcare burden, health systems are recognising the need to provide additional support and alternative models of care.
To this end, the DHHS has established the HealthLinks programme in Victoria for health services to pilot innovative models of integrated care. The DHSS disconnected funding for a select higher-risk group, replacing the activity-based model with a block fund. The goal is to encourage Victorian health services to better connect a patient’s care journey, both within the health service and in their community.
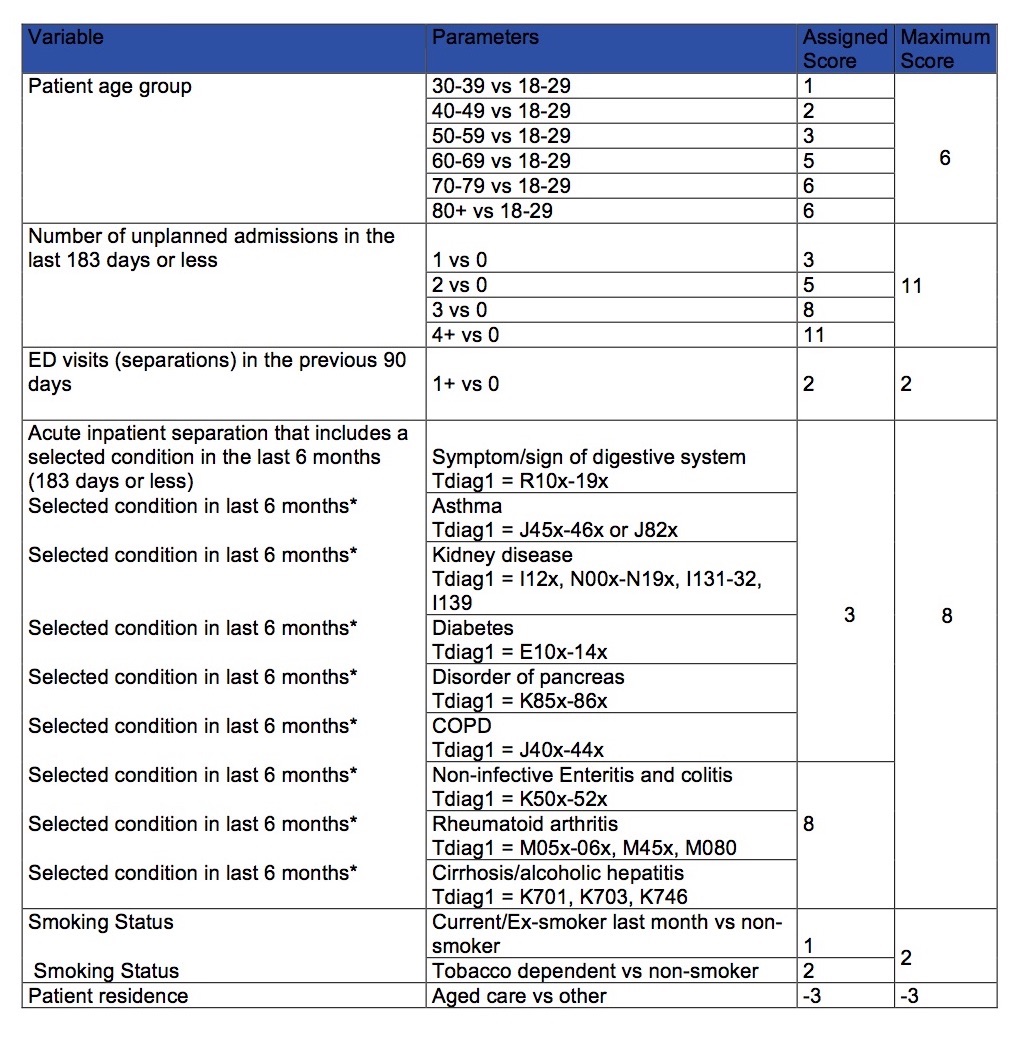
In collaboration with Australia’s Commonwealth Scientific and Industrial Research Organisation (CSIRO), and select members from Victorian health services, the DHSS has developed a statistical model that identifies a cohort of patients who are frequently being re-admitted and could, potentially, benefit from alternative service delivery models (see Appendix 1 for the HealthLinks algorithm).
The specific aims of the initiative is to determine if flexible funding enables health services to develop and implement alternative models to inpatient acute care that provide better experiences and outcomes for patients with chronic conditions, at equal or lower cost. To determine if this aim has been met, the DHHS is seeking to measure the impact on:
- the total length of stay in acute inpatient care for enrolled and intervention patients;
- the care experience of enrolled and intervention patients;
- the consumption of (state-funded) healthcare resources by enrolled and intervention patients;
- the cost of services delivered by participating services to enrolled and intervention patients; and
- the experience of the workforce involved in delivering alternative models of care.
Development of the Western HealthLinks model of care
Strategic direction
The WH Strategic Plan 2015-2020 (the Strategic Plan) had established the implementation of integrated care models as a priority for WH. Western HealthLinks is directly linked to our mission:
To provide seamless, effective and efficient care that reflects the whole of a person’s health needs; from prevention through to end of life, across both physical and mental health, and in partnership with individuals, their carers and family. This will be achieved by focusing on the person’s needs, better communication and connectivity between healthcare providers in primary care, community and hospital.
Integrated Care Committee
WH’s understanding of the need to improve the care integration for patients challenged with chronic and complex illness was stimulated through the formation of the WH Integrated Care Committee in early 2015. Highlighting the importance WH regarded this area, the committee was chaired by the chief executive officer with support from the board chair. Providing high-quality integrated community-based care and ongoing support can result in better outcomes for people living with chronic conditions, and may help reduce their need for inpatient care.4
The committee’s initial goal was to develop an understanding of how WH was performing with providing quality integrated care. An exhaustive community engagement process was conducted with more than 1000 members of the community. This engagement highlighted the significant improvement required in the areas of communication, connecting care, and increasing support provided for patients following discharge from hospital. Numerous case reviews were also conducted, which validated this feedback with several gaps identified in how we support patients to transition home, how we communicate with the next care provider, and how we assist patients to navigate a complex health system.

Following this community engagement and case review process, the WH Integrated Care Committee conducted extensive consultation and benchmarking to develop an understanding of best practice integrated care models. Examples from other jurisdictions considered include the Canterbury District Health Board in New Zealand, the United States’ Accountable Care Organisations, the care homes and vanguards system in the United Kingdom, and the integrated care programmes in Norway, Denmark and Sweden.
This research, benchmarking and consultation process revealed a number of core elements being implemented to deliver improved models of integrated care. These consistent elements were translated into what WH has termed the ten key success factors (KSFs) to providing quality care integration (Figure 2) which ultimately informed the development of the Western HealthLinks model of care (Figure 3).
The research deemed the following factors important:
- The identification of high-risk patients and ensuring these patients experience a quality transition from the hospital to their homes.5
- In relation to communication, up to two-thirds of discharged patients reported that no one at the hospital talked to them about managing their care at home, with other studies highlighting patients did not understand their discharge medications or had no understanding of their principal diagnosis. In contrast, patients who clearly understood their post-discharge plan, through strategies such as teach-back, were identified as 30-per-cent less likely to be readmitted or visit the emergency department.
- Single elements in isolation will have limited affect in providing comprehensive integration with multicomponent strategies required to achieve the desired outcomes.5 Consequently, WH has pursued the goal of implementing all ten KSFs to support the Western HealthLinks programme (KSF #10).
- Many readmission risk-screening tools are biased towards clinical factors. However, the local research conducted by WH and subsequent literature review highlighted the importance of also factoring in a patient’s psychosocial, cognitive and debility factors to provide a more comprehensive assessment of their readmission risk.6,7,8
- WH research on 30-day readmission tools highlighted that patients were less likely to engage in community programmes, such as Western HealthLinks, when an extended time period exists between their discharge from hospital to engagement about a programme or service.
Gap analysis
In developing the Western HealthLinks model of care, WH conducted a gap analysis to ascertain the ability to be able to deliver all elements of the care model. This gap analysis highlighted that while WH was able to provide various elements of the programme, there were some elements identified as requiring external support. WH engaged with the Silver Chain Group (SCG) to deliver key aspects of the innovative pilot. SCG is a major not-for-profit organisation with a proven record of delivering quality community health and aged care services across Australia.
Western HealthLinks model of care
Commencing in November 2016, the Western HealthLinks programme was established to ensure a more supportive, cohesive and integrated model of care for WH’s chronic and complex patient group with the goal of improving the care experience and providing more healthy days back in their own homes.
WH’s chronic and complex patient group is now supported through the Western HealthLinks model of care (Figure 3), which features the ten key success factors. Supporting this group across the entire health journey requires supportive, co-ordinated care and quality communication to be provided across the hospital, community and primary care phases. 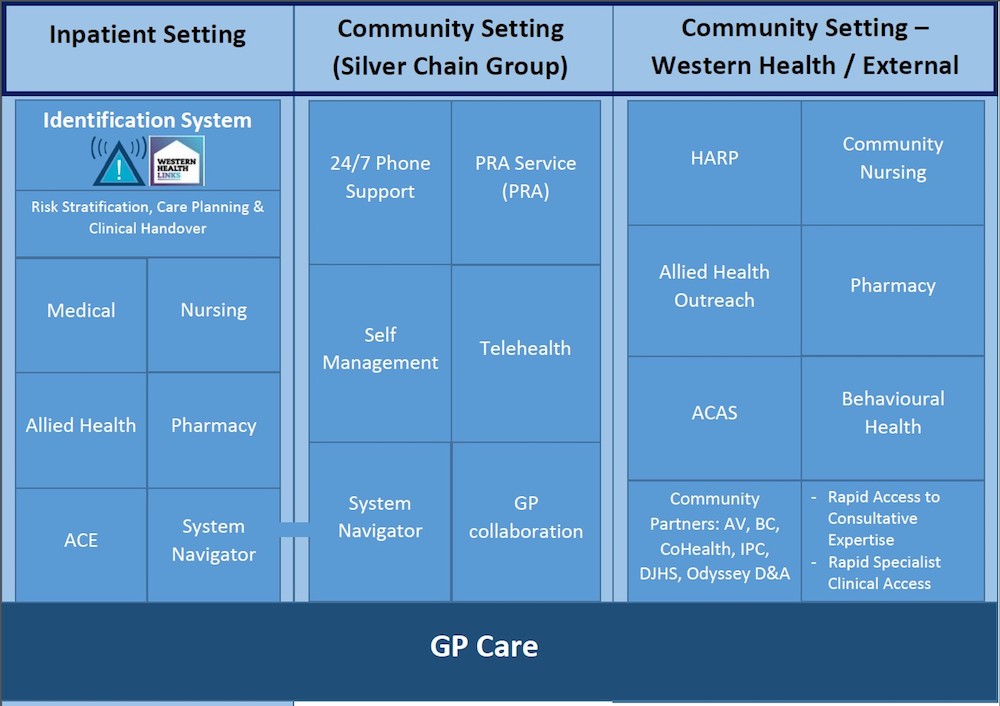
Inpatient setting
To enable the timely identification of eligible patients, WH has developed several identification systems. Prior to the development of the identification algorithm and related systems, WH was identifying less than 28 per cent of patients recognised as requiring additional support with their transition home and post-discharge care.
All qualifying patients to the programme have the Western HealthLinks alert automatically uploaded to their digital medical record, enabling clear identification of their enrolment on the programme.
Additional alerts have also been developed, which include the Western HealthLinks worklists, alerts on the ward-based electronic journey boards, medical team alerts, and text message alerts.
Following identification, it is imperative that Western HealthLinks patients have a clear care plan outlined, have their post-discharge needs assessed, and experience a quality transition from hospital to home.5 To ensure each Western HealthLinks patient receives a quality transition from hospital, a team of internal care co-ordinates has been established through the realignment of existing resources. The Advice Co-ordination and Expertise (ACE) team ensure each qualifying patient is identified and that key staff, such as medical, nursing, allied health and pharmacy, are aware so they can provide patients with a quality transition from hospital, including referral to post-discharge services based on assessment of patients’ needs.
This research informed the practice of inviting the system navigator into the hospital to engage with qualifying patients while they’re still in hospital, in order to develop an initial rapport, provide information about the programme, and establish mutually suitable times for the initial home visits. The SCG system navigator has been provided with employment status at WH, with access to all WH patient administrative systems and staff connections.
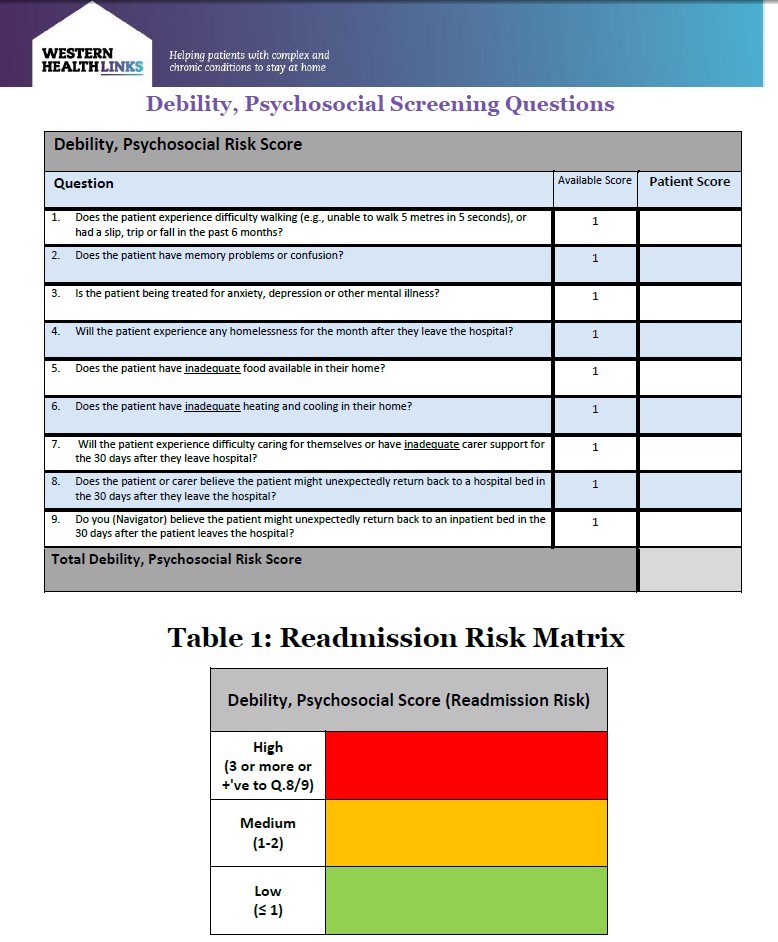
Consequently, Western HealthLinks has established additional screening with the development of an additional nine questions. Termed the ‘Western 9’ (Appendix 2), the first seven questions are designed to assess the patient’s debility, cognition, and their current housing situation and care support status. Two additional ‘surprise’ questions are also asked, with question eight acknowledging the patient’s and their carer’s understanding of their condition, and their likelihood of re-attending hospital to seek support. Question nine acknowledges the clinical team’s knowledge, education and experience to assess a patient’s risk of readmission to hospital. Responses to the Western 9 questions result in the patient being screened into either the high-, medium- or low-risk care group.
Supporting the patient’s GP by providing them with quality information and ongoing communication is of key importance. The GP is contacted when one of their patients qualifies for the programme, with feedback sought regarding their current care plan and the plan proposed by the medical unit. Often, the GP has known and cared for patients challenged with chronic and complex illness for several years, and is well placed to inform the proposed care plan and the compatibility of these care plans with the patient’s compliance level. The GP is sent the care plan via a secure electronic gateway on discharge from hospital, with the patient’s system navigator providing ongoing connection with the patient and the health service.
With the majority of patients with chronic and complex illness prescribed poly-pharmacy regimes, attempts are made to ensure each patient receives a pharmacy review and reconciliation, both while an inpatient and following discharge from hospital.
To improve patients and carer understanding of their condition and care plan, development has commenced to introduce teach-back at WH, with an initial focus on Western HealthLinks patients. Teams such as ACE ask patients if they require any additional information regarding their condition or care plan, and either educate patients in this area or facilitate connections to specialists, such as medical staff, pharmacy or allied health.
Once consenting to the programme, the patient and their carer are provided with a Western HealthLinks welcome pack, which includes information about the programme, a fridge magnet with a 24/7 phone contact number, information to support access to the clinical portal, and additional information, such as the Charter of Patient Rights.
To improve the way referrals are processed at WH, a new electronic referral system (ERS) has been developed. The ERS enables referrals to be made early on admission, with additional information to be added throughout the inpatient episode. The ERS has removed the requirement for the referrer to select a specific service or programme, instead enabling them to select the identified need, such as nursing or physiotherapy. The referrer can monitor and review when the patient has received the required care.
Furthermore, to ensure the quality management of referrals, the Central Access Unit (CAU) has been established to process and schedule all community referrals.
Community setting: provided by Silver Chain Group
Following engagement from the SCG system navigator in hospital, a system navigator also follows up with the patient in their home, with initial visits established to assess the patient’s compliance level with the Flinders Partners of Health screen, in addition to commencing the patient on their chronic disease self-management care plan, which emulates the details of their GP-facilitated chronic disease management plan. Connection is made with the patient’s GP to ensure they’re aware of their enrolment to the programme, and the patient is supported to schedule a follow-up appointment with their GP.
The system navigator provides ongoing support for patients with self-management strategies, and support to navigate the health system through facilitating connections, arranging for home-based clinical and social services, as well as support with GP and hospital-based appointments.
Patients are screened using the ‘Western 9’, with high-risk patients supported with a weekly home visit; medium-risk patients supported with a combination of a fortnightly home visit alternating with fortnightly phone support; and low-risk patients encouraged to call the 24/7 phone number to seek clinical support or system navigation, following their initial home visit, to commence them on their chronic disease self-management plan.
Patients are provided access to the clinical portal, a web-based product that patients and carers, such as their GP and health workers, can use to review clinical information and appointment schedules.
All patients are supported with access to a specific 24/7 phone number, which enables connection to a registered nurse 24 hours a day. Phone support programmes are effective in reducing readmission and improving satisfaction, especially when combined with home-based care support.9,10,11
Between the hours of 07.00 to 22.00, the phone-based registered nurse, the GP, health workers, or the patient and carer themselves can enact the priority response and assessment (PRA) service. This service involves the rapid deployment of registered nurses to the patient’s home for clinical intervention, with the support of the patient’s GP or, if they’re unavailable, the SCG GP, aiming to support the patient remain in their home.
Community setting: provided by Western Health and other community partners
Pre-existing services available to WH have been realigned to ensure the enhanced support for Western HealthLinks patients. Clinical support for specific conditions, such as chronic heart failure, COPD and diabetes, is provided by the WH’s Hospital Admission Risk Program (HARP), in addition to providing psychosocial supports in areas such as homelessness, financial burden, heating and cooling, family violence, and hoarding and squalor. Outreach services, such as nursing and allied health, are provided in the patient’s home, in addition to linking patients to supportive programmes such as drug and alcohol, and mental health. The Aged Care Assessment Service (ACAS) support a patient’s application to residential aged care services or additional homecare packages.
The system navigator facilitates connections back to WH – for example, connecting the PRA nurse or GP via phone to specialists, including cardiologists, respiratory consultants and renal physicians, in addition to facilitating rapid access to a specialist clinic review at WH, if deemed appropriate. If an inpatient admission is required, arrangements are made to support the patient’s direct admission into an inpatient bed, avoiding the need to present to the emergency department.
Governance
Programme governance
The purpose of the Western HealthLinks governance structure is to facilitate effective decision-making in the Western HealthLinks pilot programme.
This governance involves:
- domains – what decisions need to be made about the project;
- authority – who is responsible for making key decisions; and
- structures and processes – how the decision-making occurs.
The Western HealthLinks pilot programme is governed under the following committees:
- Western HealthLinks Joint Steering Committee;
- Western HealthLinks Project Management Office / Operational Committee;
- Western HealthLinks Model of Care Operational Committee; and
- SCG Western Melbourne Project Team.
Clinical governance
When working in partnership, there is an imperative to ensure that a strong and clear clinical governance framework exists between both organisations. This framework (Figure 6) outlines the roles, reporting, accountabilities, KPIs, and joint quality and safety activities that will maintain standards and allow high-quality care to be delivered.
In developing the framework, it was important to integrate governance arrangements into each organisation’s clinical governance structures. Both organisations are accredited under the National Standards Program and, as such, have strong governance arrangements. Where the services come together, joint Steering and Project Management (PMO) committees have responsibility of governance across the programme, as illustrated below. Reporting KPIs (including clinical) are covered in the service-level agreement, which is monitored via the committee structure.
Western HealthLinks: Year one evaluation
WH’s Performance Unit analysed activity over the first year of the programme (Nov 2016 – Oct 2017) with the control year at Western Health chosen to be the original programme modelling year (Nov 2014 – Oct 2015). To enable this, the DHHS algorithm was re-run against the patients enrolling in the first year of the programme, as well as against patients in the control year.
 Data analysis revealed positive results with a reduction in hospital-based activity when comparing the first year of the programme to the control year. All results were identified as having statistical significance with a p value of <.001.
Data analysis revealed positive results with a reduction in hospital-based activity when comparing the first year of the programme to the control year. All results were identified as having statistical significance with a p value of <.001.
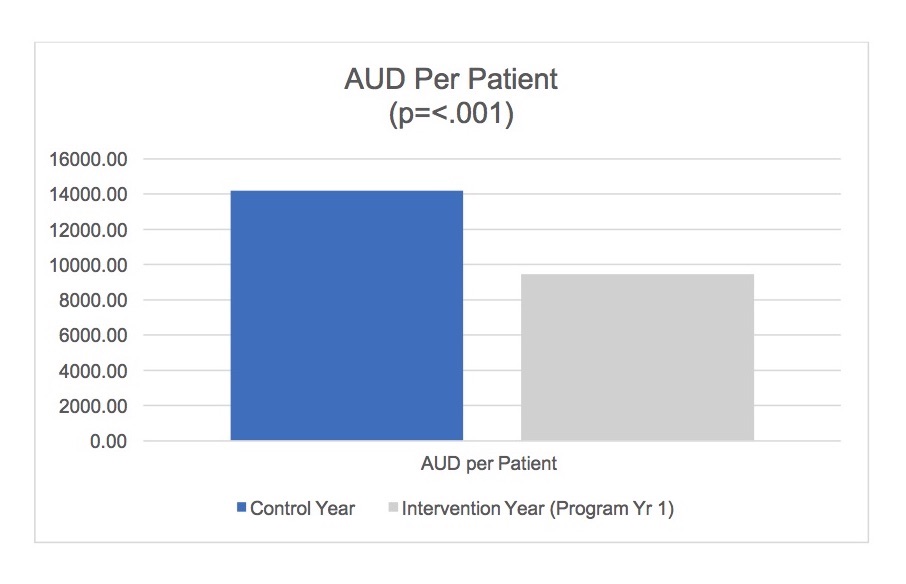
Financial evaluation
A reduction in the cost accumulated by the patients over the first year of the programme was noted, with AU $9,464 per patient in the first programme year compared with the control year of AU $14,196 – a reduction of 33 per cent. The accumulated estimated cost savings in year one of the active programme on 1859 patients amounted to AU $8,796,788.
Bed days
The average bed days per patient reduced from 9.7 to 7.5 when comparing the two years. This represents a reduction of 23 per cent, a reduction in 3961 beds over the year, or 10.9 beds per day. 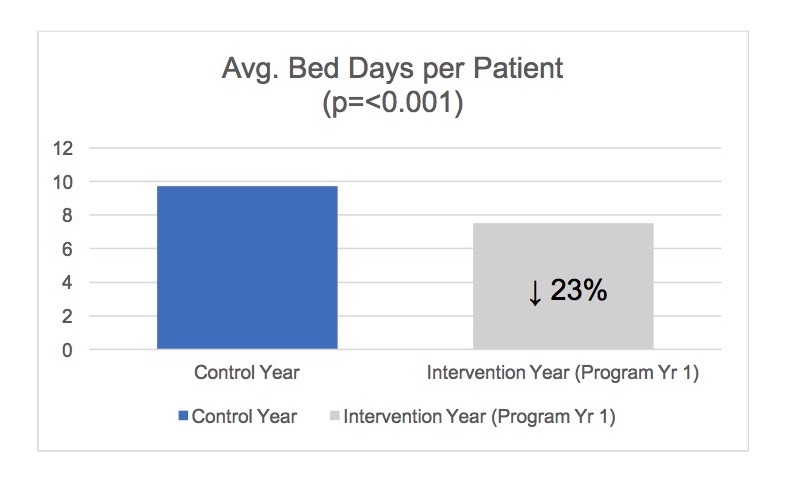
Episodes per patient
The average episodes per patient reduced from 2.34 to 1.95 when comparing the two years, representing a reduction of 17 per cent in the average episodes per patient.
Patient experience
Integral to the programme’s performance is the experience patients report while being supported on the programme. To enable the assessment of patient experience, WH developed an ethically approved research framework, with the assessment of the patient’s healthcare experience central to this assessment. 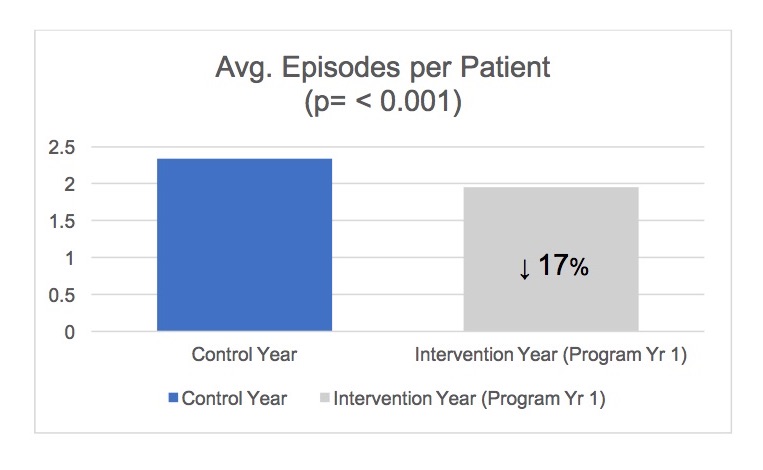
To enable this, patients are requested to complete a survey as they enrol for the programme (baseline), and then at six monthly intervals. At the time of reviewing the completed surveys, it was assessed that sufficient surveys were completed at both the baseline and at six months, however, insufficient surveys were completed at 12 months. Consequently, the patient’s experience in the one-year review paper was assessed by comparing the patient’s experience at baseline to the six-month point.
What is working well with you healthcare compared with six months ago?
The qualitative analysis highlighted a significant improvement in patient experience with their healthcare between baseline and at six months. A thematic analysis demonstrated patients have experienced improvements in how their care is co-ordinated, the quality of communication they’re receiving, the responsiveness of receiving support, and the satisfaction with receiving care in their own home as opposed to needing to attend hospital.
Services in home and local community – GPs, chemists and HealthLinks
“The daily contact, Western link [sic], being able to ring and speak to a person that has my history at hand.”
Assistance with access, co-ordination and navigation – quick responses, navigation of the system, access to appointments
“That I can call a nurse to come to my home and assess if I need to go to hospital or GP, instead of wasting time for long hours in hospital that can affect my conditions for the worse.”
Health information and communication
“Everybody was very helpful and understanding, and explained everything so I understood and were very caring.”
Areas suggested for improvement
Patients were also provided the opportunity to suggest areas of improvement, which included the request for more services to be provided in their homes, reducing wait times to hospital-based appointments, greater support to understand their condition and care plan when transitioning from hospital, and the challenges of following a care plan with the existence of a mental health condition.
Increasing home care services eg, physio programmes, homecare and transport
“Nurses to visit home. Maybe someone to drive to appointments when family members not available.”
Decrease waiting times in ED and OPD
“That when I am referred by my GP to have some tests, as I was recently to see a specialist for my kidneys care, I am on a waiting list for a very long time . . . and my health is deteriorated.”
Improve hospital facilities and car parking – including toilet and shower facilities, and provision of disability parking
“More parking for disabled at hospitals.”
Dedicated time for personal care and comfort in hospital – a sense that hospital staff are always busy
“Perhaps more volunteer workers, especially at meal times helping to open packets.”
Dedicate sufficient time in discussing the patient’s condition and what they need to do
“More targeted age-specific education and information.”
Understanding challenges of how mental health impacts on managing a chronic illness
“GPs and other healthcare professionals understanding mental healthcare as experiences, and don’t understand how hard changes are to be made.”
Conclusions
The first year of the Western HealthLinks programme has resulted in an increase in the time that qualifying patients are spending in their own homes and away from hospital, in addition to realising improvements in their overall healthcare experience. With the research indicating that results such as these are extremely unlikely in the short term, achievement of these results is extremely pleasing and provides further motivation to continually improve and embed the programme at Western Health.
Implementing the programme during the first year has not been without its challenges. The evolution of the algorithm was one such problem, with several modifications throughout the year requiring WH to respond rapidly to these alterations to ensure the accurate identification of each patient. Consequently, several patients were missed on their initial enrolment throughout the earlier part of the first year, requiring a manual enrolment process to be implemented and retrospective engagement to consent to the programme. Stabilisation of the algorithm towards the later part of the first year provided increased stability with the identification system, resulting in greater identification accuracy of patients at their indexed admission.
As the Western HealthLinks programme developed, so did the need for new systems and processes, the redesign and augmentation of existing services, and the establishment of new collaborative arrangements, such as the one established with SCG. Change management was essential to ensure the development and sustainability of these key programme areas.
The challenging workload and multiple commitments have provided the medical teams a task to ensure each Western HealthLinks patient receives a comprehensive care and transition plan. Several strategies, such as the implementation of a new electronic medical record (EMR), are being reviewed for their potential to support this area. Similarly, consistent quality engagement with the GP community is an area being continually assessed for improvement. With the patients dispersed across the western region and GP community, consistent engagement and awareness of the programme has required significant effort.
Consistent to the learnings provided through the literature review, a high proportion of patients were identified as requiring moderate to high levels of behavioural health support. Support for conditions, such as anxiety, depression, personality disorders, and drugs and alcohol, has required innovative strategies to identify existing support services or development of new approaches to support this area.
Although WH recognises further development is required to embed the model of care based on the 10 KSFs, the first year of the Western HealthLinks integrated care programme has provided a solid foundation for further development and improvement over the coming years.
Authors
A/Prof Craig Nelson is head of unit – nephrology / medical director, HealthLinks at Western Health. Robert Rothnie is director, service planning and development at Western Health. Jason Plant is programme director, HealthLinks at Western Health. Dr Arlene Wake is executive director, community integration, allied health and service planning at Western Health, and Russell Harrison is CEO.
References
- Australian Institute of Health and Welfare. 2017. http://www.aihw.gov.au/media-release-detail/?id=6012955
- Scott, IA, Shohag, H, and Ahmed, M. 2013. Quality of care factors associated with unplanned readmissions of older medical patients: a case control study. Internal Medicine Journal. Nov 2013. 161-167.
- Dr Foster Intelligence System. 2015. http://www.drfoster.com/
- Independent Hospital Pricing Authority. https://www.ihpa.gov.au/what-we-do/activity-based-funding
- Mudge, AM, Shakhovsky, R, and Karrasch, A. Quality of transitions in older medical patients with frequent readmissions: opportunities for improvement. European Journal of Internal Medicine. 2013. 24; 779-783.
- The King’s Fund. Bringing together physical and mental health. A new frontier for integrated care. https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/Bringing-together-Kings-Fund-March-2016_1.pdf
- Roberts, RS, Crigler, J, Ramirez, C, Sisco, D, and Early, GL. Working with socially and medically complex patients: when care transitions are circular, overlapping and continual rather than linear and finite. Journal for Healthcare Quality. Vol. 37, No. 4; 245-265.
- Bartels, JS, DiMilia, PR, Fortuna, KL, and Naslund, JA. (2018). Integrated care for older adults with serious mental illness and medical co-morbidity. The Psychiatric Clinics of North America. 2018. 41; 153-164.
- Johnson, BM, Laderman, M, and Coleman, EA. Enhancing the effectiveness of follow-up phone calls to improve transitions in care: three decision points. The Joint Commission Journal on Quality and Patient Safety. May 2013. Vol. 39; 221-227.
- Miller, DA, and Schaper, AM. Implementation of a follow-up telephone call process for patients at high risk for readmission. Journal of Nursing Care Quality. Vol. 30, No. 1; 63-70.
- Wong, FKY, Ching, S, Chau, J, Law, AKP, Tam, SKF, and McGhee, S. Economic evaluation of the differential benefits of home visits with telephone calls and telephone calls only in transitional discharge support. Age and Ageing. 2015. 44; 143-147.
Organisations involved