Cities / Public health
Comment
The threat of yellow fever in Asian cities
29 Mar 2021 | 0
Where Aedes mosquitoes are abundant, yellow fever is both more easily spread and probably at least four times as deadly as SARS-CoV-2. In a commentary based on a wider paper in the Cities & Health journal, Fiona C Shenton and Steve W Lindsay discuss the ongoing threat of a yellow fever pandemic and outline strategies to “build out” the mosquitoes that transmit this deadly disease.
If nothing else, the current Covid-19 pandemic has demonstrated our lack of preparedness in the face of a fast-spreading infectious disease.1 
Diseases can be transmitted directly from person to person, as well as by means of an intermediary or vector, such as a mosquito. The common urban mosquito, Aedes aegypti, has been referred to as the yellow fever mosquito because of its role in transmitting the yellow fever virus (see Fig 1).
Originally, Ae. aegypti was a tree-hole breeding mosquito found in the forests of West Africa, but it has since evolved to live in towns and cities throughout the tropics and sub-tropics. This urban environment provides an ideal habitat – a plethora of breeding sites provided by small bodies of water collected in discarded plastic, guttering and uncovered containers, and ready access to human bloodmeals.
While many people who contract yellow fever do not develop symptoms, for those who do become sick, the consequences can be severe. The early symptoms are sudden onset of fever with chills, aches and pains, severe headache, fatigue, nausea and vomiting. After three or four days of sickness most will recover, but for some, following an apparent improvement, a high fever sets in; multiple organs are affected leading to haemorrhage and shock. Liver damage causes jaundice, with the skin and whites of the eyes turning yellow – hence the name yellow fever (see Fig 2). For those who enter this second distressing stage, the mortality rate can be as high as 60 per cent.
 Yellow fever is endemic in tropical areas of Africa and Central and South America, but so far it has not spread to countries in Southeast Asia. In 2017, the World Health Organization (WHO), in partnership with UNICEF and Gavi, launched the Eliminate Yellow Fever Epidemics (EYE) Strategy. With more than 50 partners involved, the EYE partnership supports 40 at-risk countries in Africa and the Americas to prevent, detect and respond to suspected cases and outbreaks of yellow fever. Vaccination is an important component of the EYE strategy; it combines national childhood routine immunisation with preventive vaccination campaigns in high-risk areas. The yellow fever vaccine is safe and 95-per-cent effective, but there is not enough of it to cover those living in countries where the disease is endemic, let alone outside these regions.
Yellow fever is endemic in tropical areas of Africa and Central and South America, but so far it has not spread to countries in Southeast Asia. In 2017, the World Health Organization (WHO), in partnership with UNICEF and Gavi, launched the Eliminate Yellow Fever Epidemics (EYE) Strategy. With more than 50 partners involved, the EYE partnership supports 40 at-risk countries in Africa and the Americas to prevent, detect and respond to suspected cases and outbreaks of yellow fever. Vaccination is an important component of the EYE strategy; it combines national childhood routine immunisation with preventive vaccination campaigns in high-risk areas. The yellow fever vaccine is safe and 95-per-cent effective, but there is not enough of it to cover those living in countries where the disease is endemic, let alone outside these regions.
Following a yellow fever outbreak in Angola in 2015–2016, which spilled over into neighbouring countries, the WHO increased its stockpiles of the vaccine to 18 million doses. During this outbreak, there were several reports of Chinese workers infected with the virus returning to their home country. Had the disease spread in the wider region, where very few of its 1.8 billion people are either vaccinated or immune, the outcome could have been catastrophic. And the vehicle for such spread would have been the mosquito Ae. aegypti.
In the map below (see Fig 3), the grey areas show the potential global distribution of Ae. aegypti, and the red dots are cities with more than 1 million inhabitants; it shows clearly the level of threat to India and cities in Southeast Asia. Not only are people in the region not naturally immune to the disease but a recent study has shown that Southeast Asian strains of Ae. aegypti are just as capable as other strains of taking up the yellow fever virus and passing it on from one person to another when they take bloodmeals.2

What has all this to do with healthy city design? Recognising the impossibility of ever having sufficient vaccine to cover all those at risk, an essential arm of the EYE strategy is mosquito control and protection from mosquito bites. The BOVA Network (https://www.bovanetwork.org/) is a broad coalition of vector-control experts and practitioners from the built environment. Its primary focus has been in countries in sub-Saharan Africa, where the burden of diseases transmitted by mosquitoes is greatest, but the principles apply worldwide.
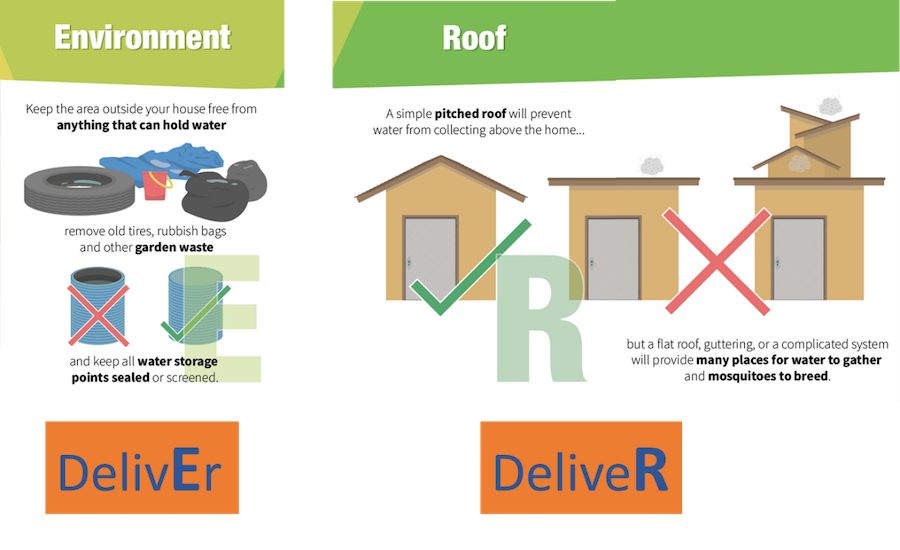
It has recently published recommendations for “building out” mosquitoes.3 Some of these recommendations relate to house modifications, which reduce the number of mosquitoes entering indoors. However, Aedes mosquitoes mostly bite during the daytime both indoors and out, so the best way to control them is to remove all potential breeding sites from within and around the house. Aedes mosquitoes lay their eggs in small bodies of water, which can readily collect in any manner of small containers, including flower pots, uncovered stored-water containers, discarded waste such as plastic bottles and old tyres outdoors, and in guttering or culverts underground. Provision of a reliable, clean water supply without leaks will therefore ensure there is no need to store water and no pooling around taps and pipes. Collecting solid waste will also help, as will designing structures that prevent water from collecting (see Fig 4). For these measures to be most effective, a multi-sectoral approach is essential, with homeowners, municipal authorities, town planners, builders and others all having a role. Singapore has instigated a truly impressive dengue control programme, relying on such measures.4 Dengue virus is also transmitted by Aedes mosquitoes and it’s the fastest growing infectious disease after Covid-19. Singapore’s National Environment Agency takes overall responsibility for controlling this disease, but multiple stakeholders are involved with clear lines of command and regular communication between the different parties.
In Cities & Health5 – the partner journal of the Healthy City Design 2020 International Congress, at which the findings of this research were presented – the recommendations were set in the context of the WHO’s Global Vector Control Response (GVCR) 2017–20306 and the United Nations’ Sustainable Development Goals7, notably Goal 3: Good Health and Wellbeing, Goal 11: Sustainable Cities and Communities, and Goal 17: Partnerships for the Goals. City leaders have played a key role in responding to the Covid-19 pandemic. They have first-hand knowledge of the situation in their locality, plus oversight and responsibility for local services. They are best placed to manage similar threats from other infectious diseases.
A yellow fever pandemic must be avoided at all costs. By taking the approach advocated above, not only can we protect against mosquito-transmitted diseases, such as yellow fever and new diseases that may threaten us in the future, but at the same time we can enhance people’s overall health and wellbeing by providing a safe and comfortable place to live.
Summary
- Asia is home to cities with millions of people.
- The mosquito Aedes aegypti is abundant in cities and towns throughout the region. It is the world’s most efficient transmitter of arboviruses, including yellow fever, which kills 20-60 per cent of people who fall sick with the disease.
- Few people in Asia are immune or vaccinated against yellow fever; while a very effective vaccine exists, supplies fall well short of what would be required to cover the total population potentially at risk.
- A yellow fever pandemic in an Asian city would claim thousands of lives.
- WHO recommends that mosquito populations should be controlled by combining good environmental management to reduce their aquatic habitats, including the provision of reliable piped water and effective waste management, with housing improvements to prevent mosquitoes entering dwellings.
- Effective control relies on strong multi-sectoral collaboration, with co-operation between those in the health and built environment sectors.
- City leaders are ideally placed to co-ordinate disease prevention and control. It’s important that they are supported in this role.
A more detailed paper by the authors is available in the Cities & Health journal.
References
- Horton, R. The Covid-19 catastrophe: what’s gone wrong and how to stop it happening again. Cambridge, UK: Polity Press; 2020.
- De Guilhem de Lataillade, L, Vazeille M, Obadia T, et al. Risk of yellow fever virus transmission in the Asia-Pacific region. Nat Commun, 11(5801); 2020. doi: https://doi.org/10.1038/s41467-020-19625-9
- Lindsay, SW, Davies, M, Alabaster, G, Altamirano, H, Jatta, E, Jawara, M, Carrasco-Tenezaca, M, von Seidlein, L, Shenton, FC, Tusting, LS, Wilson, AL, and Knudsen, K. Philosophical transactions B Opinion piece on: Recommendations for building out mosquito-transmitted diseases in sub-Saharan Africa: the DELIVER mnemonic (in press).
- Sim, S, Ng, LC, Lindsay, SW, and Wilson, AL. A greener vision for vector control: the example of the Singapore dengue control programme. PLOS Neglected Tropical Diseases, 14(8), e0008428; 2020. doi: https://doi.org/10.1371/journal.pntd.0008428
- Shenton, FC, and Lindsay, SW. Preventing yellow fever epidemics in Asian megacities: how can cities control mosquito-transmitted diseases? Cities & Health. Taylor & Francis; 2021. https://doi.org/10.1080/23748834.2021.1899486
- World Health Organization. Global Vector Control Response 2017–2030. Geneva: WHO; 2017.
- UN. 2017 New urban agenda. Habitat III, Quito, 17-20 October 2016. United Nations’ conference on housing and sustainable urban development. New York: UN. See http://habitat3.org/the-new-urban-agenda/
About the authors
Fiona C Shenton is BOVA network facilitator at the University of Durham. Steve W Lindsay is professor of public health entomology at the same university.
Acknowledgements
The authors are supported by the Global Challenges Research Fund (GCRF) for the Building Out Vector-borne diseases in sub-Saharan Africa (BOVA) Network (www.bovanetwork.org), which is co-funded by the Biotechnology and Biological Sciences Research Council (BBSRC), Medical Research Council (MRC), and Natural Environment Research Council (NERC) of the UK. Grant BB/R00532X/1.
Organisations involved
